Vasovagal syncope is usually benign and self-limiting, but can be life-threatening if not managed properly.
Loss of consciousness, however brief in duration, can produce physiologic changes and place the patient's life in danger.
Predisposing Factors
Psychogenic Factors
- Fright, anxiety and emotional stress.
- Sudden or unexpected pain.
- Sight of blood and surgical or dental instruments eg, syringe and needle.
Non-psychogenic Factors
- Sitting in an upright position or standing.
- Hunger from fasting or missed meals.
- Exhaustion.
- Poor physical condition.
- Hot, humid, crowded environment.
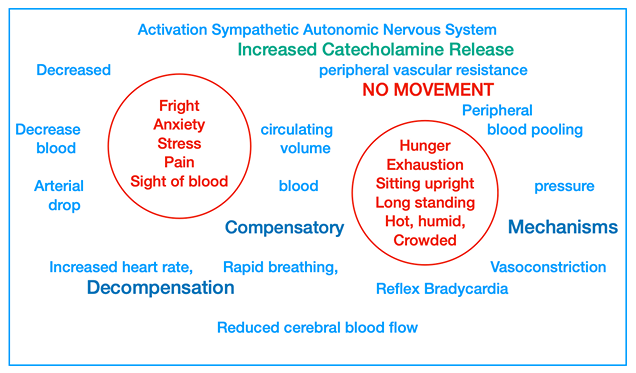
Pathophysiology
In vasovagal syncope, there is activation of the sympathetic division of autonomic nervous system, that incites a fight-or-flight response and release of increased amounts of catecholamines, epinephrine and norepinephrine into the blood.
This leads to a decrease in peripheral vascular resistance and diversion of large amount of blood into the skeletal muscles.
-
In normal fight-or-flight response, the blood is pumped back to the heart from peripheral tissues, due to muscular activity.
-
However, patients cannot run from the dental chair, instead, they remain seated while the dental procedures are performed, which causes pooling of blood in the extremities, with lesser volume of blood returning to the heart.
-
As a result, there is a relative decrease in circulating blood volume, drop in arterial blood pressure and a decreased in cerebral blood flow.
-
As the blood pressure begins to fall, compensatory mechanisms are activated to increase the cardiac output, maintain close-to-normal blood pressure and ensure adequate cerebral blood flow. These includes:
- Baroreceptor reflex: Constricts peripheral blood vessels to increase the return of venous blood to the heart.
- Carotid and aortic arch reflexes: Increases the heart rate.
-
However, if the situation goes unmanaged, there is fatigue (decompensation) of these compensatory mechanisms and development of reflex bradycardia (slowing of heart rate to less than 50 beats per minute).
-
This is associated with significant drop in cardiac output and fall in blood pressure to levels below those critical for maintenance of consciousness. Hence, cerebral ischemia occurs and consciousness is lost.
-
Cerebral ischemia lasting only 10 seconds can lead to seizure activity and convulsive movements of the arms and legs.
-
The consciousness is regained with improvement in cerebral blood flow and can be hastened by positioning the patient in supine position with legs elevated, which increases venous return to the heart.
Clinical Manifestations
Presyncope
- Feeling of warmth in the neck and face, pallor or ashen-gray skin color.
- Cold sweat, primarily on the forehead.
- Feeling bad or faint and nauseous.
- Pupillary dilation.
- Yawning and Hyperapnea (increased depth of respiration)
- Coldness in hand and feet.
- Disturbed vision and dizziness.
- Significant increase in heart rate (initially), followed by hypotension and bradycardia at later stage.
Syncope
- Loss of consciousness.
- Irregular, jerky breathing, that is quiet, shallow and rarely perceptible.
- Respiratory arrest or apnea.
- Pupillary dilation and a deathlike appearance.
- Convulsive and muscular twitching of the hands, legs or facial muscles.
- Bradycardia (Heart rate of 50 beats per minute or less)
- Weak and thready pulse.
- Generalised muscle relaxation, may cause partial or complete airway obstruction.
- Fecal or urinary incontinence may occur, particularly when the systolic BP falls below 70 mm Hg.
Post-syncope
- Pallor, Nausea, Weakness and Sweating.
- Confusion or disorientation.
Management
Step 1: Positioning
- All current dental procedures should be stopped immediately.
- Vital signs should be taken and any dental instrument left in the patient's mouth should be removed.
- The patient should be placed in a Trendelenburg position (supine position with legs slightly elevated).
- The patient should be asked to move their feet and fingers as much as possible, so as to pump blood back to the heart.
Step 2: Assessment of Circulation, Airway and Breathing (CAB)
- Particularly important if there is loss of consciousness i.e, the patient has gone into syncope.
- Circulation: Carotid pulse is palpated -> Weak, thready carotid pulse is palpable in most circumstances.
- Airway: The adequacy of an airway can be determined by the use of look-listen-feel technique. The oral cavity should be examined to rule out any blockage. A patent airway is successfully established by the head tilt-chin lift procedure.
- Breathing: Can be assessed by observing the chest movements and listening or feeling the exhaled air. Spontaneous respiration is usually evident during syncope, however, rescue breathing may be necessary in cases where spontaneous breathing ceases.
Step 3: Definitive Care
- Oxygen administration: At a rate of 4-6 L/min via nasal cannula or 10 L/minute via mask.
- Blood pressure, heart rate and respiratory rate should be monitored, recorded and compared to the patient's preoperative baseline values to determine the severity of the reaction and degree of recovery.
- Tight clothes such as ties, collars and belts (can decrease blood flow to brain) should be loosened.
- Respiratory stimulant such as aromatic ammonia is useful, if the patient is hypoventilating and is slow to recover consciousness. Inhalation of ammonia, which has noxious odor, stimulates both increased breathing and muscular movement.
- A cold towel may be placed on the forehead of a patient who is warm or blankets can be provided for petients feeling cold.
- If bradycardia persists, an anticholinergic, such as atropine, may be considered.
- If hypoglycemia is suspected, raw sugar or in the form of juice can be administered.
- If the consciousness is not regained for more than a minute, a different cause for syncope should be considered and the emergency medical system should be activated.
Post-syncope measures
- As the patient becomes conscious, the doctor and emergency team must maintain their composure, and the stimulus the precipitated the syncope should be removed from the patient's sight.
- The patient should not undergo any further treatment after recovery for the day.
- The precipitating event or other factors eg, hunger or fear must be determined before sending the patient home.
- The patient should not leave the dental office without a responsible adult escort (preferably, a family member) to accompany the patient home.
- Future visits by the patient must be planned with preoperative sedation and additional anxiety reduction protocols.
Points to Note
- Synonyms: Neurogenic, Neurocardiogenic or Neurally mediated syncope, Psychogenic syncope, Atrial Bradycardia, Swoon, Benign, Simple or Common faint.
- If the patient is in upright position, presyncope can lead to unconsciousness in a relatively short time (apprx 30 seconds), while in supine position, presyncope might never progress to syncope.
- Look-listen-feel: look to see if the chest is moving; listen for wheezing, indicative of a partial airway obstruction, or no sound, indicating complete airway obstruction; feel that there is little or no air exchange.
- The effect on blood pressure, by placing an unconscious, hypotensive patient into supine position is equivalent to the intravenous administration of 2 L fluid.
- The critical level of cerebral blood flow for maintenance of consciousness is about 30 ml of blood per 100g of brain tissue per minute. The human adult brain weighs approximately 1360g and the normal cerebral blood flow is 50-55 ml per 100g per minute. In normotensive individual, this is equivalent to systolic blood pressure of 70 mm Hg.
References
- Medical Emergencies in the Dental Practice (7th Edition), Stanley F. Malamed, Daniel L Orr II, Mosby Elsevier.
- Medical Emergencies in Dental Practice, Orrett E. Ogle, Harry Dym, Robert J. Weinstock, Quintessence Publishing Co, Inc.
- Medical Emergencies Essentials for the Dental Professional (2nd Edition), Ellen B. Grimes, Pearson Education Inc.
*This article is an excerpt from the above mentioned books and Medical Sutras does not make any ownership or affiliation claims.