It is the 10th cranial nerve that is composed of both motor and sensory fibres (mixed nerve).
- Longest and most widely distributed cranial nerve.
- Has an extensive vague course and distribution, hence, the name vagus.
- Vagrant or wandering nerve with field of distribution extending beyond the head and neck to the thorax and abdomen.
- Conveys most of the efferent fibres to the cranial part of the parasympathetic outflow and distributes the fibres of cranial part of the accessory nerve.
Functional Components
Special Visceral Efferent Fibres
- Arise from the nucleus ambiguus.
- Supplies the muscles of palate, pharynx, and larynx.
General Visceral Efferent Fibres
- Arise from the dorsal nucleus of vagus.
- Provides parasympathetic innervation to heart, bronchial tree, and most of the g.i. tract.
Special Visceral Afferent Fibres
- Carries taste sensations from the posterior most part of the tongue and epiglottis.
- Terminate in the nucleus tractus solitarius.
General Visceral Afferent Fibres
- Carry general sensations from the mucous membrane of pharynx, larynx, trachea, esophagus, and thoracic and abdominal viscera.
- Terminate in the nucleus tractus solitarius and some in the dorsal nucleus of the vagus.
General Somatic Afferent Fibres
- Carries general sensations from skin of the auricle.
- Terminate in the nucleus of the spinal tract of the trigeminal nerve.
Anatomy & Pathway
Origin: The vagus nerve arises from the lateral aspect of the medulla between the olive and inferior cerebellar peduncle by about 10 rootlets below and in line of the rootlets of the glossopharyngeal nerve.
Intracranial Course
-
The nerve rootlets unite to form the nerve trunk which runs laterally, crosses the jugular tubercle, and leaves the cranial cavity.
-
It passes through the middle part of the jugular foramen enclosed in the common dural sheath with the accessory nerve.
-
In the jugular foramen, the superior and inferior sensory ganglion are located.
- Superior ganglion: Contains cell bodies of GSA fibres.
- Inferior (nodose) ganglion: Contains cell bodies of visceral afferent fibres.
-
The cranial root of accessory nerve unites with the vagus nerve just below the inferior ganglion and transfers all its fibers to the vagus nerve for distribution.
Extracranial Course
- After exiting the cranial cavity through the jugular foramen, the nerve runs vertically downward within the carotid sheath in the neck between the internal jugular vein (laterally) and internal and common carotid artery (laterally).
- The right vagus nerve enters the thorax by crossing in front of the right subclavian artery, while the vagus nerve enters the thorax by passing between the left common carotid and left subclavian arteries.
Branches & Distribution
Branches of Superior Ganglion
- Meningeal Branch: Takes a recurrent course, and enters the cranial cavity through the jugular foramen, and, supplies the dura mater of the posterior cranial fossa.
- Auricular Branch (Arnold's/Alderman's Nerve): Supplies the floor of the meatus and the tympanic membrane.
Branches of Inferior Ganglion
-
Pharyngeal Branch: Takes part in the formation of pharyngeal plexus, and, supplies all the muscles of pharynx except stylopharyngeus and all the muscles of soft palate except, tensor palati.
-
Branches to carotid body
-
Superior laryngeal nerve (Nerve of 4th arch): Divides into external and internal laryngeal nerves:
- External laryngeal nerve (motor): Supplies cricothyroid and gives twigs to the inferior constrictor and pharyngeal plexus.
- Internal laryngeal nerve (sensory): Carries sensation from the mucous membrane of larynx above the vocal cords and of the pharynx, epiglottis, vallecula, and posterior most part of the tongue.
Branches in the Neck
- Superior & Inferior Cervical Cardiac Branch: Carry preganglionic parasympathetic fibres to the heart and are cardio-inhibitory.
- Recurrent Laryngeal Nerve (Nerve of 6th arch): Provides motor supply to all the intrinsic muscles of the larynx (except, cricothyroid), and, sensory supply to the mucous membrane of laryngeal cavity up to the vocal cord.

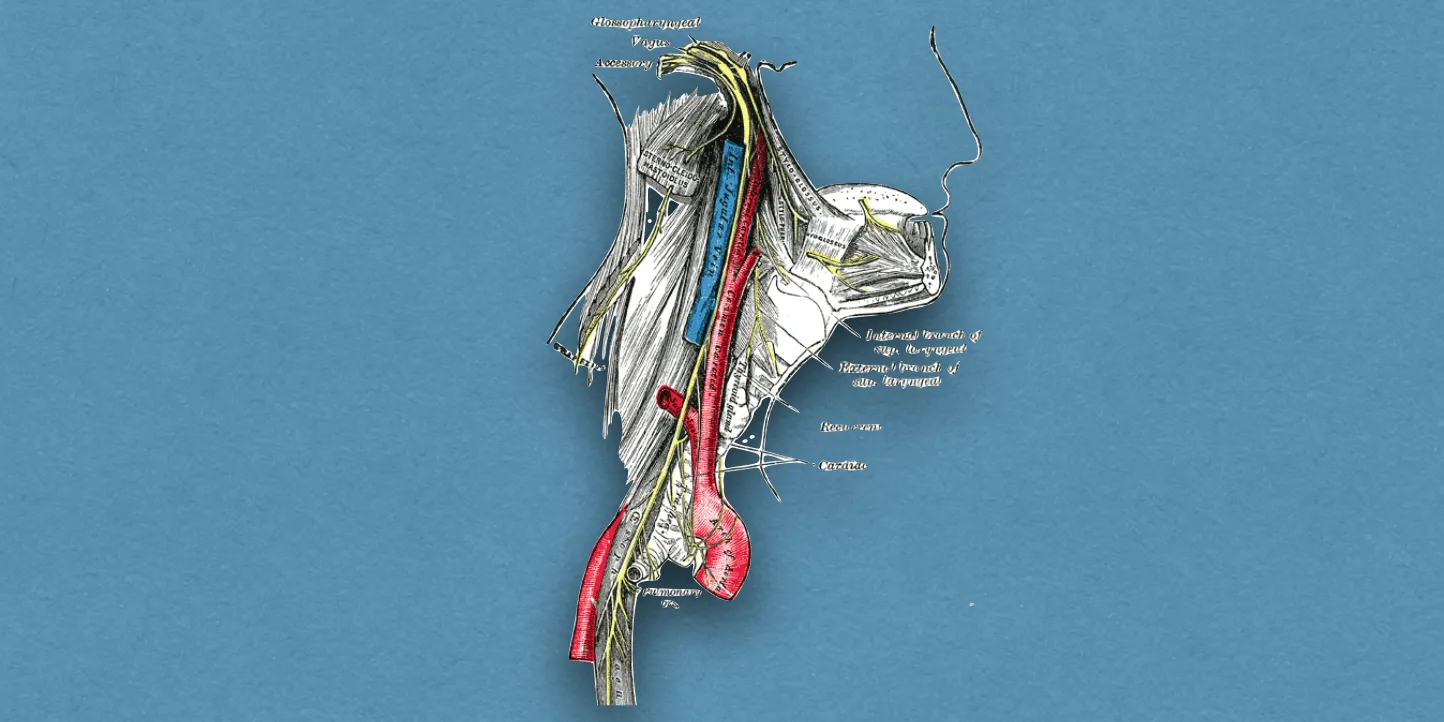
Image Credit: Jkwchui (Source: Based on on drawing by Truth-seeker2004, Creative Commons Attribution-Share Alike 3.0 Unported license.)
{kind=link}
Clinical Significance
The bilateral lesions of vagus nerve causes:
- Nasal regurgitation of the swallowed liquids.
- Nasal twang of voice.
- Hoarseness of voice.
- Flattering of palatal arches.
- Cadaveric position of vocal cords.
- Dysphagia.
- Loss of cough reflex.
Clinical Testing of Vagus Nerve
- Method: Ask the patient to open his/her mouth and say 'ah' and compare the palatal arches of the two sides.
- Normal: The soft palate rises (elevated) in the midline, if the vagus is intact.
- Unilateral lesion: Flattening (drooping) of palate arch on the paralysed side and pulling of uvula to the normal side.
- Bilateral lesions: Soft palate drops.
*Alderman's Nerve Phenomenon
- There is stimulation of jaded appetite by tickling of the cutaneous distribution (auricular branch) of the vagus nerve.
- It's stimulation may cause reflex coughing (ear cough), vomiting, and even cardiac arrest.
References
| [](https://amzn.to/3Ixnict)
Textbook of Anatomy Head, Neck, and Brain (Volume III), Vishram Singh |
- The image used in the cover photo is in public domain (Source: Wikimedia Commons).
*This article is an excerpt from the above mentioned sources and Medical Sutras does not make any ownership or affiliation claims.