Ulcerative colitis (UC) is a mucosal disease that usually involves the rectum and extends proximally to involve all or part of the colon. The different presentations of UC includes,
- Limited to rectum and rectosigmoid : 40-50%.
- Extends beyond the sigmoid but not involving the whole colon : 30-40%.
- Pancolitis : 20%.
- Backwash ileitis : Involves inflammation of 2-3 cm of the terminal ileum (in 10-20% cases), due to backwash of colonic content into the terminal ileum in case of pancolitis.
Montreal Classification of Extent and Severity of UC
-
Extent
- E1 (Ulcerative proctitis) : Involvement limited to the rectum.
- E2 (Left-sided UC / Distal UC) : Involvement limited to the colorectum distal to to the splenic flexure.
- E3 (Extensive UC / Pancolitis) : Involvement extends proximal to the splenic flexure.
-
Severity
- S0 (Clinical remission) : Absence of symptoms.
- S1 (Mild disease activity) : Less than 4 stools per day (with or without blood), absence of systemic illness, normal inflammatory markers (ESR).
- S2 (Moderate disease activity) : More than 4 stools per day but minimal signs signs of systemic toxicity.
- S3 (Severe disease activity) : More than 6 bloody per day, pulse more than 90 beats/min, temperature more than 37.5 oC, hemoglobin less than 10.5 g/100ml and ESR more than 30 mm/h.
Macroscopic features
- Mild inflammation : Mucosa is erythematous with a fine granular surface that look like sandpaper.
- Severe cases : Mucosa is hemorrhagic, edematous and ulcerated.
- Long-standing cases : Inflammatory polyps (pseudopolyps) may be present as a result of epithelial regeneration.
- Fulminant disease : Toxic colitis or megacolon may develop where the bowel wall becomes thin and the mucosa is severely ulcerated. This may lead to perforation.
- Remission : Mucosa may appear normal.
- Patients with many years of disease : Mucosa appears atrophic and featureless and the entire colon becomes narrowed and shortened.
Histologic findings
The disease process is limited to the mucosa and superficial submucosa, with deeper layers unaffected except in fulminant disease. The two major histologic features that suggest chronicity and help distinguish UC from infectious or acute self-limited colitis include,
- First, the crypt architecture of the colon is distorted, crypts may be bifid and reduced in number, often with a gap between the crypt bases and the muscularis mucosa.
- Second, some patients have basal plasma cells and multiple basal lymphoid aggregates. Mucosal vascular congestion, with edema and focal hemorrhage, and an inflammatory cell infiltrate of neutrophils, lymphocytes, plasma cells and macrophages may be present.
- The neutrophils invade the epithelium usually in the crypts and give rise to cryptitis and ultimately to crypt abscesses.
Clinical presentation
-
Major symptoms : Diarrhoea (often nocturnal and/or post-prandial), rectal bleeding, tenesmus, passage of mucus and crampy abdominal pain (the severity of symptoms correlates with the extent of disease).
-
Proctitis :
- Patients usually pass fresh blood or blood-stained mucus, either mixed with stool or streaked onto the surface of a normal or hard stool.
- Have tenesmus, or urgency with a feeling of incomplete evacuation.
- Slow proximal transit (may account for the constipation seen in patients with distal disease).
-
Disease extending beyond the rectum :
- Blood is usually mixed with stool or there is grossly bloody diarrhoea.
- Altered colonic motility due to inflammation, with rapid transit through the inflamed intestine.
- When the disease is severe, patients pass a liquid stool containing blood, pus and fecal matter.
-
Pain :
- Severe pain is not a prominent symptom. Severe cramping and abdominal pain can occur with severe attacks of the disease.
- Some patients with active disease may experience lower abdominal discomfort or mild central abdominal cramping.
-
Other symptoms : Anorexia, nausea, vomiting, fever and weight loss.
-
Physical signs
- Proctitis : Tender anal canal and blood on rectal examination.
- More extensive disease : Tenderness to palpation directly over the colon.
- Toxic colitis : Severe pain and bleeding.
- Megacolon : Hepatic tympany.
- Perforation : Signs of peritonitis.
Investigations
Diagnosis relies on the patient's history, clinical symptoms, negative stool and/or tissue examination for bacteria, C. difficile toxin, ova and parasites, and viruses depending on epidemiologic considerations and clinical presentation; sigmoidoscopic appearance; and histology of rectal or colonic biopsy specimens.
Fecal lactoferrin and calprotectin are used frequently to rule out active inflammation versus symptoms of irritable bowel or bacterial overgrowth.
-
Active disease : Can be associated with an increase in acute phase reactants (C-reactive protein, CRP), platelet count and ESR, and a decrease in hemoglobin.
-
Fecal lactoferrin : A glycoprotein present in activated neutrophils, is a highly sensitive and specific marker for detecting intestinal inflammation.
-
Fecal calprotectin : Present in neutrophils and monocytes, and levels correlate well with histologic inflammation, predict relapses, and detect pouchitis.
-
Severely ill patients : Quick fall in the serum albumin level.
-
Leukocytosis may be present but is not a specific indicator of disease activity.
-
CRP : Rise is CRP is rarely seen in proctitis or proctosigmoiditis.
-
Sigmoidoscopy : Used to assess disease activity and is usually performed before treatment.
-
Colonoscopy : Used to assess disease extent and activity, if the patient is not having an acute flare.
-
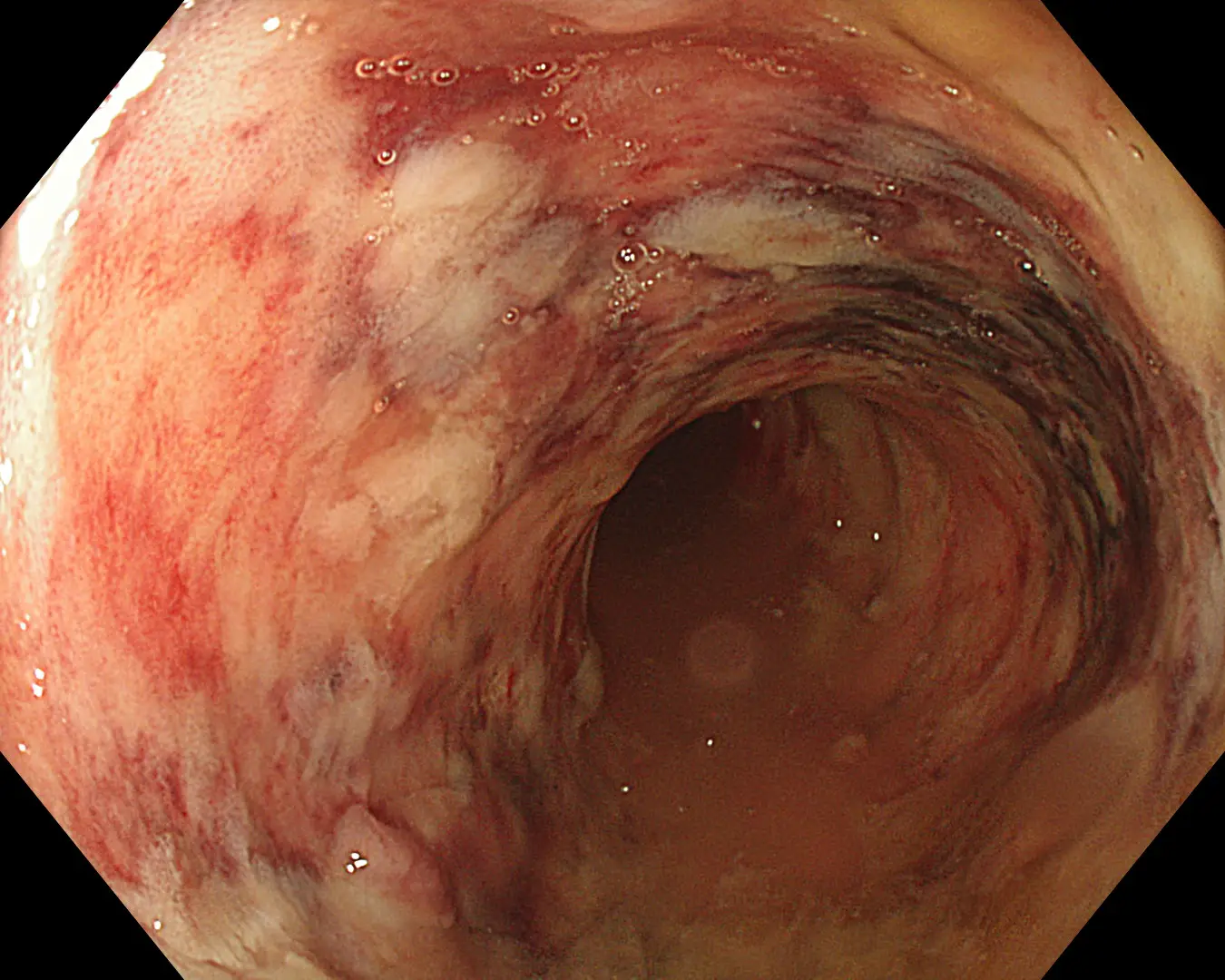
Endoscopy :
- Mild disease : Erythema, decreased vascular pattern, and mild friability.
- Moderate disease : Marked erythema, absent vascular pattern, friability, and erosions.
- Severe disease : Spontaneous bleeding and ulcerations.
-
Radiologic changes : Earliest changes seen on single contrast barium enema is a fine mucosal granularity and, with increasing severity, the mucosa becomes thickened and superficial ulcers are seen. Deep ulcerations can appear as 'collar-button' ulcers, which indicate that the ulceration has penetrated the mucosa.
Complications
-
Massive hemorrhage : Occurs in 1% of patients, treatment of the disease usually stops the bleeding.
-
Toxic megacolon : Defined as a transverse or right colon with a diameter of more than 6cm, with loss of haustration, seen in patients with severe attacks of ulcerative colitis.
-
Perforation : Most dangerous of the local complications, the physical signs of peritonitis may not be obvious, esp. if the patient is receiving glucocorticoids.
-
Strictures :
- Always a cause of concern in UC, as there is possibility of underlying neoplasia.
- Strictures that are impassable with the colonoscope should be presumed malignant until proven otherwise and are indication for surgery.
-
Occasional complications : Anal fissures, perianal abscesses, or hemorrhoids (the occurrence of extensive perianal lesions should suggest Crohn's disease).
References
- Harrison's Principles of Internal Medicine (21st edition), Loscalzo, Fauci, Kasper, Hauser, Longo, Jameson, The McGraw-Hill Companies.
- The image used in the cover is licensed under the Creative Commons Attribution-Share Alike 4.0 International license. Author : Federica Viazzi (A0 AL), Source : Own Work (Wikimedia commons).
*This article is an excerpt from the above mentioned book and Medical Sutras does not make any ownership or affiliation claims.