Dental caries is caused primarily by an imbalance of the oral flora (biofilm) due to the presence of fermentable dietary carbohydrates on the tooth surface over a period of time. However, several factors are involved in the process and not all individuals with teeth, biofilm and consuming carbohydrates develop dental caries.
Primary Modifying Factors
- Tooth anatomy.
- Saliva.
- Biofilm pH and composition.
- Use of fluoride.
- Dietary habit.
- Oral hygiene.
- Immune System.
- Genetic factors.
Secondary modifying factors
- Socioeconomic status.
- Education.
- Lifestyle.
- Environment.
- Age.
- Ethnicity.
- Occupation.
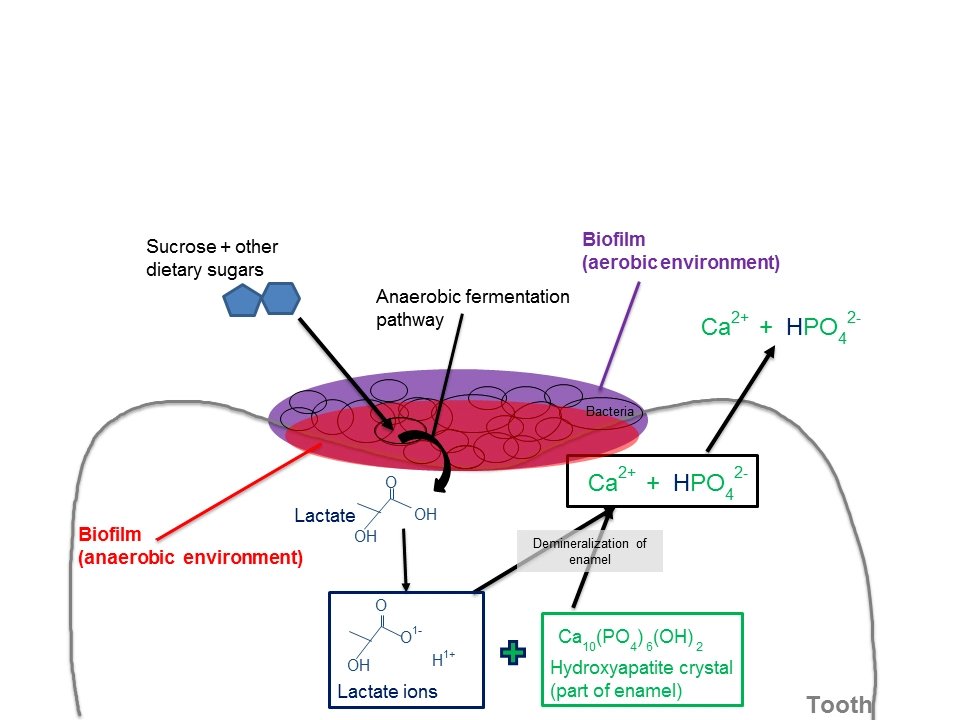
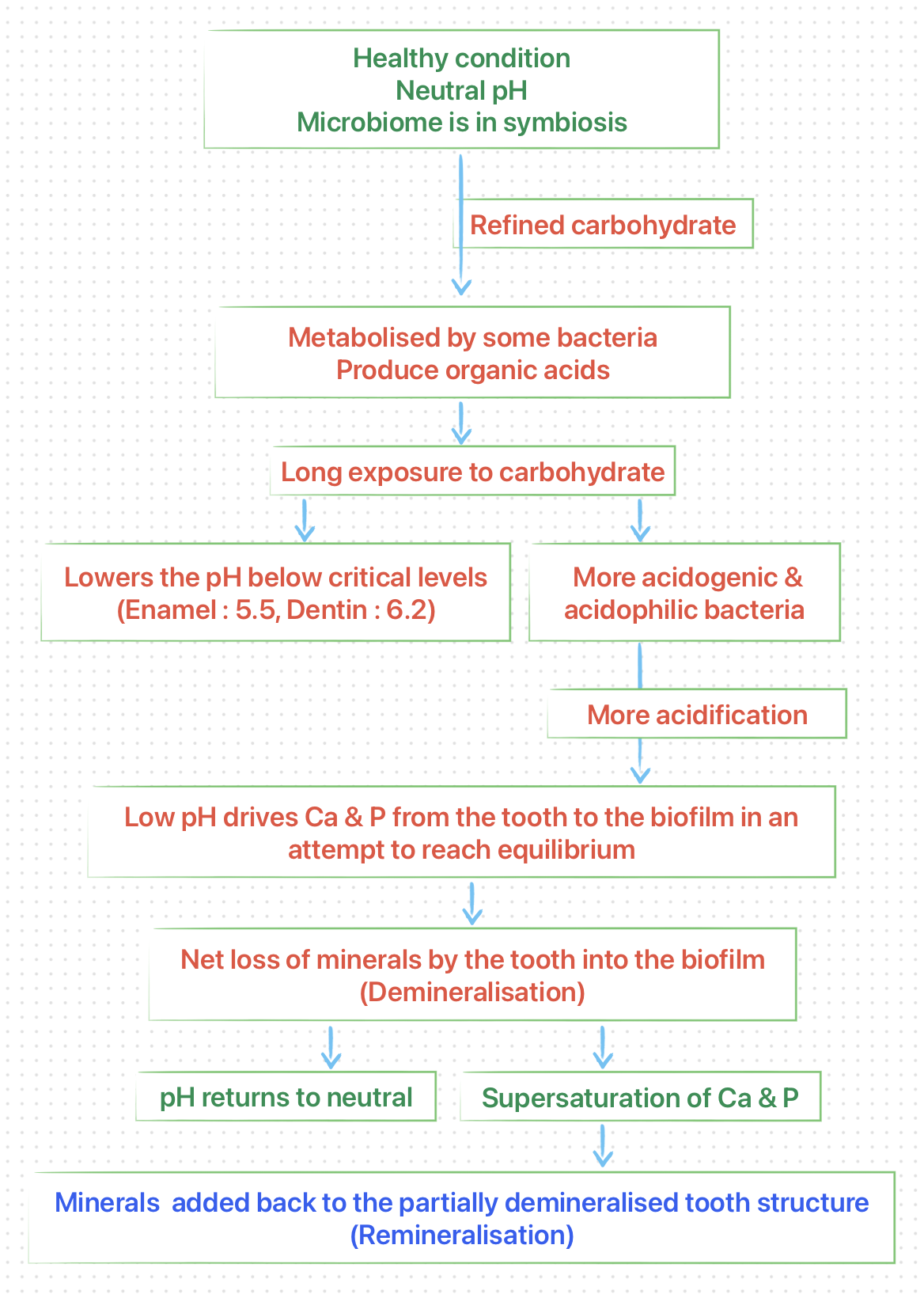
The development of dental caries may be considered as a continuous dynamic process that involves repeating periods of demineralisation by organic acids of microbial origins and subsequent remineralisation by salivary components (or therapeutic agents), but in which the overall oral environment is imbalanced toward demineralisation.
 Demineralisation
Demineralisation
-
Demineralisation refers to loss of mineral salts (inorganic components of the hard tissues of the tooth).
-
The acids involved in the demineralisation are normal metabolic byproducts of the microorganisms and are generated by the metabolism of carbohydrates. The microorganisms involved include aciduric and acid tolerant streptococci, lactobacilli, diphtheroids, yeasts, staphylococci, and certain strains of sarcinae.
-
The outer surface of enamel is far more resistant to demineralisation by acid than is the deeper portion of enamel, so, the greatest amount of demineralisation occurs 10-15 micrometer beneath the enamel surface. The continuation of this process results in the formation of an incipient subsurface enamel lesion that is first observed clinically as white spot.
-
The subsurface lesion continues to enlarge, with the eventual collapse of the surface and formation of cavitation in the enamel surface, unless the demineralisation is arrested or reversed (remineralisation).
-
Demineralisation of dentin mineral (inorganic phase) results in exposure of the protein matrix, followed by denaturation and degradation of the organic phase (primarily dentin collagen), leading to dentin cavitation.
-
The outcome of demineralisation depends on the oral environment and may result in :
- Arrested lesion: Arrested caries (enamel), Eburnated dentin (dentin),
- Reversal of caries, or
- Cavitation.
-
The pathological factors favouring demineralisation:
- Acid-producing bacteria.
- Sub-normal saliva flow and/or function.
- Frequent eating/drinking of refined, fermentable carbohydrate.
- Poor oral hygiene.
Remineralisation
It refers to the replacement of the mineral content of the body (or part of the body), after it has been disrupted by the demineralisation process (or disease). It occurs by re-precipitation of calcium and phosphate ions released by subsurface dissolution.
-
In the oral cavity, remineralisation of the incipient subsurface lesions may occur as long as the surface layer of the enamel remains intact.
-
In this process, breathed air containing carbon dioxide mixed with saliva (containing H2O) forms an unstable carbonic acid that dissolves minerals, forming mineral ions.
-
Saliva that is supersaturated with calcium and phosphate ions and has acid-buffering capacity, diffuses into plaque, where it neutralises the microbial acids. The calcium and phosphate ions, then, precipitates to solid state and are incorporated on the demineralised tooth surface.
-
Factors are to be considered in this process include,
- A molecule of carbonic acid must be present.
- Carbonic acid should be near the remineralisation spot (No food debris).
- Remineralisation spot should be clear.
- Carbonic acid again changes to CO2 and H2O (whenever there is excess).
- Sufficient mineral in saliva.
-
The protective factors favouring remineralisation include,
- Saliva flow and components.
- Presence of fluoride, calcium and phosphate.
- Good oral hygiene.
- Strategies that maintain a healthy microbiome (probiotics, prebiotics (arginine), pH modifiers, erythritol and xylitol).
- Strategies that modulate a dysbiotic microbiome (silver, peptides, tin, antimicrobials).
Points to Note
-
Dental caries is a multifactorial, preventable disease, classified by the FDI as a non-communicable disease.
-
Dysbiosis: Refers to diseases related to imbalances between microorganisms and the host. (Dental caries is a dysbiosis).
-
Sugar is the main stress factor that may alter the stability and promote dysbiosis.
-
Remineralisation and Age of the biofilm
- Biofilm developed for 12 hours or less: Demineralised enamel resulting from a single exposure to sucrose, can be remineralised by saliva within about 10 minutes.
- Biofilm older than 48 hours or more: At least 4 hours required for the saliva to repair the damaged enamel.
References
- McDonald and Avery's Dentistry for the Child and Adolescent, Jeffrey A. Dean, Mosby (2021)
- Sturdevant’s Art and Science of Operative Dentistry, Andre V. Ritter, Mosby (2018).
- The file used as the cover image is licensed under the Creative Commons Attribution-Share Alike 4.0 International license. Author : Alsheik4 (Wikimedia commons).
*This article is an excerpt from the above mentioned books and Medical Sutras does not make any ownership and affiliation claims.