Acute asthmatic episode occurs in patients with history of asthma and is characterised by shortness of breath or wheezing (respiratory distress), due to respiratory smooth muscle spasm (reversible), airway inflammation with edema and mucus hypersecretion (irreversible).
Pathogenesis
Acute asthmatic episode commonly occurs during or after injection or during a stimulating dental procedure such as extraction and induction/ recovery from sedation.
Normally, the tone of bronchial smooth muscles is regulated by the vagus nerve (causes constriction when stimulated) and the sympathetic nervous system (causes bronchodilation).
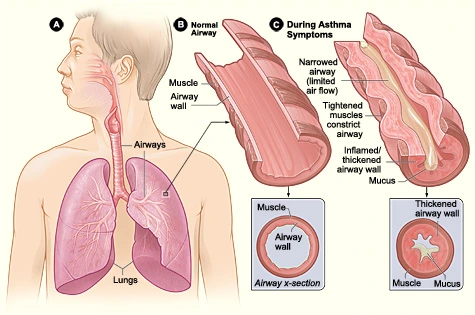
In asthmatic patients, bronchi become highly reactive with an exaggerated response of the bronchial smooth muscles (bronchospasm) to normally non-noxious stimuli. This causes narrowing of the bronchi and a restricted exchange of oxygen and carbon dioxide in the lungs.
- This leads to respiratory distress and shortness of breath as less air passes through the airway.
- As the air passes through a contracted bronchus, this creates a sound described as wheezing.
- There is air trapping within the lungs, which makes the patient sit up and use accessory muscles of respiration, so as to lift the entire rib cage and generate high negative intrapleural pressure.
- An increased level of catecholamines in the blood leads to rise in blood pressure and anxiety.
Clinical Manifestations
-
Feeling of thickness or congestion in the chest.
-
Cough (with or without sputum).
-
Shortness of breath and patient wants to sit erect or stand up.
-
Wheezing (audible during both inspiration and expiration).
-
Use of accessory muscles of respiration (Sternocleidomastoid and Scalenus muscles).
-
Tachypnea (More than 20 breaths per minute).
-
Increased blood pressure and heart rate (More than 120 beats per minute in severe cases).
-
Increased anxiety and apprehension.
-
Associated symptoms (Noted with respiratory distress) :
- Diaphoresis.
- Agitation.
- Somnolence or confusion.
- Cyanosis.
- Soft tissue retraction in the intercostal and supraclavicular regions.
- Nasal flaring.
-
If the condition worsens and bronchospasm progresses, there may be hypoxia, cyanosis and eventual loss of consciousness.
Management
-
Terminate all dental procedures.
-
Place the patient in the most comfortable position (erect or semi-erect).
-
Assess Circulation, Airway and Breathing and calm the patient.
-
Administer bronchodilator (eg. Albuterol) :
- Patient should be allowed to self-administer, if possible, using their own inhaler or from the emergency kit.
- The best route of administration is via inhalation of aerosolized spray : Have similar onset of action (within 15 minutes) but minimum systemic absorption and side effects.
- Repeated doses should be administered with caution, to avoid any overdose.
-
Administer oxygen.
-
Monitor vital signs.
If Signs & Symptoms Relieved
- Monitor in the dental office until recovery and seek medical advice before starting any further treatment.
If Signs & Symptoms Continue
- Administer Epinephrine: 0.3ml of 1:1000 IM or SC (If three doses of aerosolized bronchodilator fails to resolve the acute episode).
- Administer IV fluid (crystalloid solution 30 ml per hour).
- Monitor vital signs.
Signs & symptoms are not Relieved
- Call for medical help.
- Administer Theophylline (250 mg IV over 10 minutes) and Hydrocortisone (100mg IV).
- Shift the patient to a hospital.
Selecting a Bronchodilator
The most potent and effective bronchodilators are beta-2 adrenergic agonists such as Albuterol (Salbutamol), Epinephrine, Isoproterenol and Metaproterenol.
- Albuterol is the bronchodilator of choice for dental emergency kit: It is selective and fast-acting with long duration of action and minimal side effects. It is also recommended to treat acute asthma in patients with concomitant medical problems.
- Side effects are primarily related to the beta-1 and beta-receptor stimulating action of epinephrine and isoproterenol. Metaproterenol is partially selective beta-2 agonist with little or no beta-1 and alpha stimulating properties.
- Epinephrine is contraindicated in asthmatic patients with concomitant high blood pressure, diabetes mellitus (Induces hyperglycemia), hyperthyroidism and ischemic heart disease.
- Asthmatic children: Often relieved when removed from the treatment environment. If not, then a bronchodilator (eg. albuterol) should be administered. If this also fails, consider using epinephrine (0.15mg for weight upto 30 kg to 0.3mg for weight more than 30kg).
* Salbutamol is the International Nonproprietary Name (INN), while Albuterol is the United States Adopted Name (USAN).
Status Asthmaticus
- It is an acute exacerbation of asthma that remains unresponsive to initial treatment with bronchodilators (3 doses).
- It is a true medical emergency, which if not managed promptly, may lead to death due to hypotension and respiratory acidosis, secondary to hypoxemia and hypercapnia.
Chronic Obstructive Pulmonary Disease
Patients with COPD may also present with respiratory distress while undergoing dental treatment. It is of particular concern since, if excessive oxygen is administered to a COPD patient, it may lead to fall in respiratory rate, cyanosis and apnea.
- They become accustomed to high arterial CO2 levels and use low oxygen levels as the primary stimulus to drive respiration.
- They rely on accessory muscles of respiration for breathing and experience breathing difficulty when placed in supine position as it interferes with the use of these accessory muscles.
Points to Note
-
ASA categorisation in asthmatic patients;
- ASA 2: Well-controlled and easily managed asthma.
- ASA 3: Acute asthma precipitated by stress or exercise or requiring hospitalisation for treatment.
- ASA 4: Asthmatic symptoms present at rest.
-
The best time to treat an asthma patient is late morning or late afternoon.
-
Systemic corticosteroids are proven treatment for the inflammatory component of asthma and the onset of their anti-inflammatory effects is 6-12 hours.
-
Glucocorticoids are considered important in the management of severe acute asthma for patients aged more than 40 years.
-
Dyspnea (Air hunger) : A subjective sense of shortness of breath or difficulty in breathing.
-
Hyperpnea: Greater than normal ventilation rate, that just meets metabolic demands.
-
Tachypnea: Greater than normal respiratory rate.
-
Orthopnea: Inability to breathe except in the upright position.
-
Hyperventilation: Ventilation that exceeds metabolic demands, PaCO2 less than 35 mm Hg.
-
Hypoventilation: Ventilation that does not meet metabolic demands, PaCO2 more than 45 mm Hg.
-
PaCO2: Arterial carbon dioxide tension (Normal : 35-45 mm Hg).
-
PaO2: Arterial oxygen tension (Normal 75-100 mm Hg).
References
- Medical Emergencies in the Dental Practice (7th Edition), Stanley F. Malamed, Daniel L Orr II, Mosby Elsevier.
- Contemporary Oral and Maxillofacial Surgery (6th Edition), James R Hupp, Edward Ellis III, Myron R Tucker, Mosby Elsevier.
- Medical Emergencies in Dental Practice, Orrett E. Ogle, Harry Dym, Robert J. Weinstock, Quintessence Publishing Co, Inc.
- The image used is available in the public domain (Source: Wikimedia Commons).
*This article is an excerpt from the above mentioned books and Medical Sutras does not make any ownership or affiliation claims.