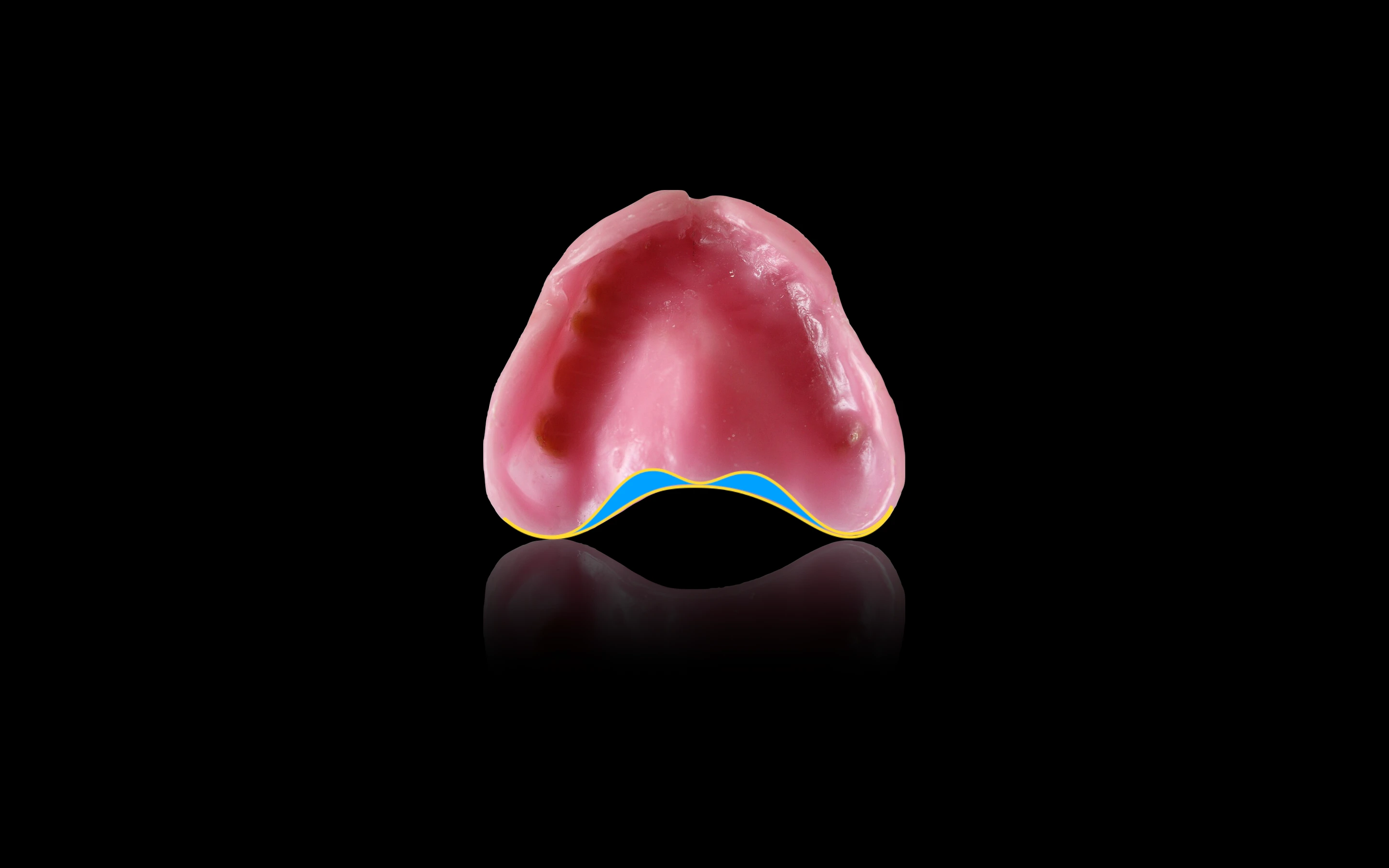
Posterior palatal seal (PPS) can be defined as that portion of the intaglio surface of a maxillary removable complete denture, located at its posterior border, which places pressure, within physiologic limits, on the posterior palatal seal area of the soft palate.
It ensures intimate contact of the denture base to the soft palate and improves retention of the denture.
The posterior palatal seal area is the soft tissue area limited posteriorly by the distal demarcation of the movable and non-movable tissues of the soft palate and anteriorly by the junction of the hard and soft palates on which pressure, within physiologic limits, can be placed.
Function
The primary purpose of PPS is to provide peripheral seal and aid in retention of the maxillary denture. This is achieved by maintaining contact with the anterior portion of the soft palate during functional movements as mastication, swallowing and phonation. Other functions include:
- Prevent separation of the denture base and soft palate during function and hence, reduce patient awareness and gag reflex.
- Reduce food accumulation beneath the posterior aspect of the denture, by proper utilisation of the compressibility of soft palate.
- Reduce patient discomfort when contact occurs between the dorsum of the tongue and the posterior end of the denture base.
- Compensate for the volumetric shrinkage that occurs during the polymerisation of the acrylic resin.
Anatomic Considerations
The posterior palatal seal is divided into two separate but confluent areas based upon anatomic boundaries.
- Postpalatal seal : Extends medially from one maxillary tuberosity to the other.
- Pterygomaxillary seal : Extends laterally through the pterygomaxillary notch (hamular notch) and continues antero-laterally for 3-4 mm approximating the mucogingival junction.
The posterior palatal seal area lies between the anterior and posterior vibrating lines.
- Anterior vibrating line : An imaginary line located at the junction of the attached tissues overlying the hard palate and the movable tissues of the immediately adjacent soft palate. It should not be confused with the anatomic junction of the hard and soft palate.
- Posterior vibrating line : An imaginary line at the junction of the aponeurosis of the tensor veli palatini muscle and the muscular portion of the soft palate. It represents the demarcation between that part of the soft palate that has limited or shallow movement (quivers) during function and the remainder of the soft palate that is markedly displaced during functional movements. It also marks the most distal extension of the denture base.
Technique
There are several techniques for the recording and placement of PPS, each having certain advantages and disadvantages.
Conventional approach
It involves the placement of PPS in the trial denture base after an accurate and fully extended final impression and cast has been made.
Steps
- Outlining the pterygomaxillary seal : The patient is seated in an upright position and instructed to rinse the mouth with an astringent to remove any stringy saliva. The posterior palatal area is then dried with gauze and a T burnisher or mouth mirror is used to palpate the hamular processes. Once located, they should be marked with an indelible pencil or noted visually. The T burnisher or mouth mirror is then placed along the posterior angle of the tuberosity until it drops into the pterygomaxillary notch. A line is placed with an indelible pencil through the notch and extended 3-4 mm anterolaterally to the tuberosity, approximating the mucogingival junction. The same procedure is then performed on the other side.
- Marking the posterior vibrating line :The patient is asked to say "ah" in short bursts in an unexaggerated fashion and the posterior vibrating line is marked by observing the movement of the soft palate.
- Delineating the posterior denture extension : The posterior vibrating line is connected with the line through the pterygomaxillary seal, thus demarcating posterior extension of the denture.
- Transfer of marking : The patient is instructed to keep the mouth open to prevent smudging of the markings, while the acrylic or shellac tray is inserted into the patient's mouth and seated firmly in place. Upon removal from the mouth, the indelible lines should be transferred to the tray. The tray is then returned to the master cast to complete the transfer of the posterior border.
- The resin tray is trimmed with a carbide bur, while shellac tray can be trimmed with a hot knife to approximate the posterior denture border.
- Marking and transfer of anterior vibrating line : The palatal tissues anterior to the posterior border are palpated with the T burnisher or mouth mirror to determine their compressibility in width and depth. The anterior vibrating line can be located using the Valsalva maneuver or asking the patient to say "ah" with short vigorous bursts. The line is marked with an indelible marker and transferred to the master cast (similar to posterior vibrating line).
- Scraping the cast : The cast is scraped to a depth of about one half the amount to which the palatal tissues in that area can be compressed, tapering progressively shallower anteriorly until it feathers out along the anterior vibrating line. A Kingsley scraper is used to score the cast. The deepest area is usually scraped to a depth of 1-1.5 mm and is located on either side of the midline, one-third the distance anterior to the posterior vibrating line. The median palatal raphe area is scraped to a depth of approximately 0.5-1.0 mm, since the tissue covering the area have little submucosa and cannot withstand the same compressive strength as the tissues lateral to it.
- Modifying the trial denture base : A shellac tray is heated and readapted on the master cast to conform with the scored PPS area, while in case of acrylic tray, small amount of self-curing resin can be added to the tray.
- Evaluation and confirmation : The tray is tried in the mouth to evaluate the contact and retention of the trial denture base. The patient is again instructed to say "ah" in short, unexaggerated manner and the posterior border is observed using a mouth mirror. If no space is noted between the trial base and the soft palate, it implies an adequate seal is achieved. However, if the soft palate separate from the trial base, further scrapping of the cast is indicated. The procedure is repeated until there is no separation between the base and soft palate.
Advantages
- The trial base will be more retentive and hence, help in getting more accurate maxillomandibular relation.
- The clinician will be able to determine the retentive qualities if the finished denture, leaving nothing to chance at the insertion appointment.
Disadvantages
- Not a physiologic technique, depends on accurate transfer of vibrating lines and careful scraping of the cast.
- There is high potential for overcompression of the soft palate.
Fluid wax technique
The indelible transfer markings are recorded on the final wash impression.
Steps
- Similar steps are followed to locate and transfer the anterior and posterior vibrating lines to the final impression.
- Waxes that flow at mouth temperature such as Iowa wax, Korecta wax No. 4, H-L physiologic paste or Adaptol are used.
- The melted wax is painted onto the impression surface within the outline of the PPS area. It is applied slightly in excess of the estimated depth and allowed to cool below mouth temperature to increase its consistency and make it more resistant to flow.
- The impression is carried to the mouth and held in place under gentle pressure for 4-6 minutes to allow the wax to flow.
- The position of the head and tongue is of particular importance during the fluid wax technique. The head is flexed such that the Frankfort plane is 30o below the horizontal and the tongue is firmly positioned against the mandibular anterior teeth. The allows the soft palate to be recorded in the most functionally depressed position.
- After 4-6 minutes, the impression is removed from the mouth and examined for uniform contact throughout the PPS area. The wax will appear dull if tissue contact has not been established, otherwise, it will have a glossy appearance. If the wax appear dull, more wax should be applied and the procedure repeated.
- The impression should also be examined to see if the wax terminates in a feather edge near the anterior vibrating line. If a butt joint is present, it means the proper flow has not taken place and the impression tray should be reinserted. Any excess wax that protrudes from the end of the tray should be removed with hot scalpel.
- The patient should be cautioned against rinsing with cold water, while the impression is out of the mouth, since, this will cause contraction of the tissues and reduce the flow properties of the wax upon insertion.
Advantages
- Physiologic technique, displaces the tissues within their physiologically acceptable limits.
- Less chance of overcompression of the soft palate.
- Mechanical scraping of the cast is avoided.
Disadvantages
- More chairside time during the impression appointment.
- Difficulty in handling the materials, and extra care is required during the boxing procedure.
Points to Note
-
The correctly placed PPS should neither impinge upon the nondisplaceable tissues of the hard palate, nor limit the muscular movements of the soft palate.
-
PPS should create a partial vacuum beneath the maxillary denture, that is activated only when horizontal or tipping forces are directed against the denture base.
-
Arbitrary scraping of master cast : It is the least accurate technique and relies upon the doctor's ability to recollect the palatal configuration and tissue compressibility.
-
House described three classifications of soft palate, based on the angle it makes with the hard palate.
- Class I : The soft palate drapes gently horizontally as it extends posteriorly and have minimal muscular activity. It remains horizontal on phonation for several millimeters posterior to the vibrating line that can be contacted and slightly displaced at rest and in function. This results in a broader surface area for contact and retention of the denture. Hence, it is considered the most favorable configuration.
- Class III : The soft palate presents the most acute contour in relation to the hard palate, and severe and immediate elevation of the soft palate almost coincident with the vibrating line. It is usually associated with a high V-shaped palatal vault. The anterior and posterior vibrating lines are separated by a few millimeters, resulting in a smaller area. The border extension in this area must be more exacting and should have almost no length posterior to the vibrating line. otherwise the border seal will be broken.
- Class II : It includes those palatal contours that lie somewhere between class I and class III.
References
- Essentials of Complete Denture Prosthodontics, 2nd edition, Sheldon Winkler, AITBS Publishers India.
- The Glossary of Prosthodontic Terms, 9th edition, The Journal of Prosthetic Dentistry.
- Prosthodontic Treatment for Edentulous Patients Complete Dentures and Implant-supported Prostheses (13th edition) , Zarb, Hobkirk, Eckert, Jacob, Mosby Elsevier.
*This article is an excerpt from the above mentioned books and Medical Sutras does not make any ownership and affiliation claims.