The permanent mandibular canine bears close resemblance with the permanent maxillary canine. Some of the differentiating features of lower canine are:
- Crown is narrower mesiodistally.
- Crown is longer by 0.5-1.0 mm in most instances, but the root is usually somewhat shorter.
- Labiolingual diameter of crown and root is usually a fraction of a millimeter less.
- Lingual surface of crown is smoother, with less development of cingulum and less bulk to the marginal ridges.
- Lingual portion of crown resembles the lingual form of mandibular lateral incisors.
- Cusp is not as well developed and cusp ridges are thinner labiolingually.
- Cusp tip is usually on a line with the center of the root, from the mesial or distal aspect.
Chronology
- First evidence of calcification: 4-5 months.
- Crown completion: 6-7 years.
- Eruption: 9-10 years.
- Root completion: 12-14 years.
Dimensions
- Overall length: 26.0 mm.
- Crown length: 11.0 mm.
- Root length: 16.0 mm.
- Mesiodistal diameter of crown: 7.0 mm.
- Mesiodistal diameter of crown at cervix: 5.5 mm.
- Labiolingual diameter of crown: 7.5 mm.
- Labiolingual diameter of crown at cervix: 7.0 mm.
- Cervical line curvature (Mesial): 2.5 mm.
- Cervical line curvature (Distal): 1.0 mm.
Crown Morphology
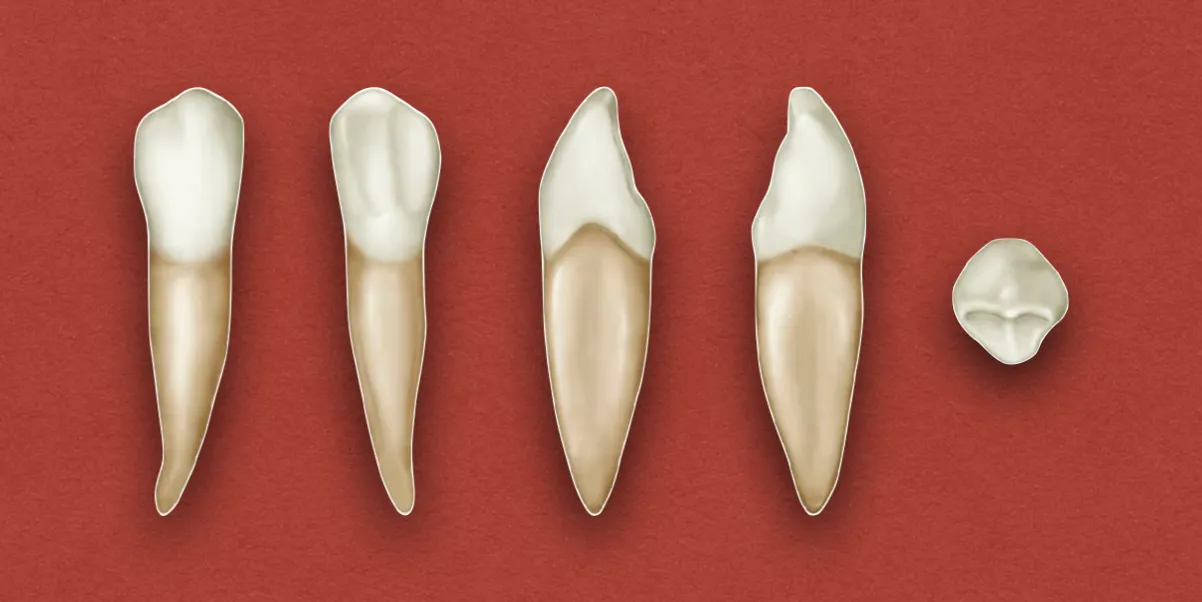
Labial Aspect
- The crown appear longer, and the mesiodistal dimensions are about 1 mm less than those of permanent maxillary canine.
- Mesial outline is almost straight with the mesial outline of the root, and the mesial contact area is near the mesioincisal angle.
- Distal contact area is more toward the incisal aspect than that of upper canine, but not up to the level of mesial contact area.
- Cervical line have a semicircular curvature apically.
- The cusp angle is on a line with the center of the center of the root, and the mesial cusp ridge is shorter.
- Many of the lower canines give the impression of being bent distally on the root base.
Lingual Aspect
- Lingual surface is smooth and regular. It is flatter, similar to the lingual surfaces of lower incisors.
- Cingulum is smooth and poorly developed.
- Marginal ridges and lingual ridge are less distinct, except toward the cusp tip, where the lingual ridge is raised.
Mesial Aspect
- Labial outline: Shows less curvature, with very little curvature directly above the cervical line (less than 0.5 mm).
- Lingual outline: Have similar curvature as the maxillary canine, but differs in degree. The cingulum is not as pronounced.
- Incisal portion: Thinner labiolingually, which makes the cusp appear more pointed and the cusp ridge more slender.
- Cusp tip: More nearly centered over the root, with a lingual placement in some cases (comparable to incisal ridges on mandibular incisors).
- Cervical line: Curves more toward the incisal portion than that of maxillary canine.
Distal Aspect
- Mostly similar to the distal aspect of maxillary canine.
Incisal Aspect
- Mesiodistal dimension is less than the labiolingual dimension.
- Mesial surface outline is less curved, when compared to maxillary canine.
- Cusp tip and mesial cusp ridge are more likely to be inclined in lingual direction, as compared to distal cusp ridge and contact area.
Root Morphology
Labial Aspect
- The root is on average 1 or 2 mm shorter than that of maxillary canine.
- Apical end is more sharply pointed.
- Root curvatures are infrequent and the curvature of root end is often in mesial direction if present.
Lingual Aspect
- Lingual portion is relatively narrower than that of the maxillary canine.
- It narrows down to little more than half the width of the labial portion.
Mesial Aspect
- The root tip is more pointed than the maxillary canine.
- Developmental depression is more pronounced and sometimes quite deep.
Distal Aspect
- Mostly similar to the distal aspect of maxillary canine, except for a more pointed root tip.
References
- Wheeler's Dental Anatomy, Physiology and Occlusion(2019), Stanley J. Nelson DDS MS, Elsevier.
*This article is excerpt from the above mentioned book and Medical Sutras does not make any ownership and affiliation claims.