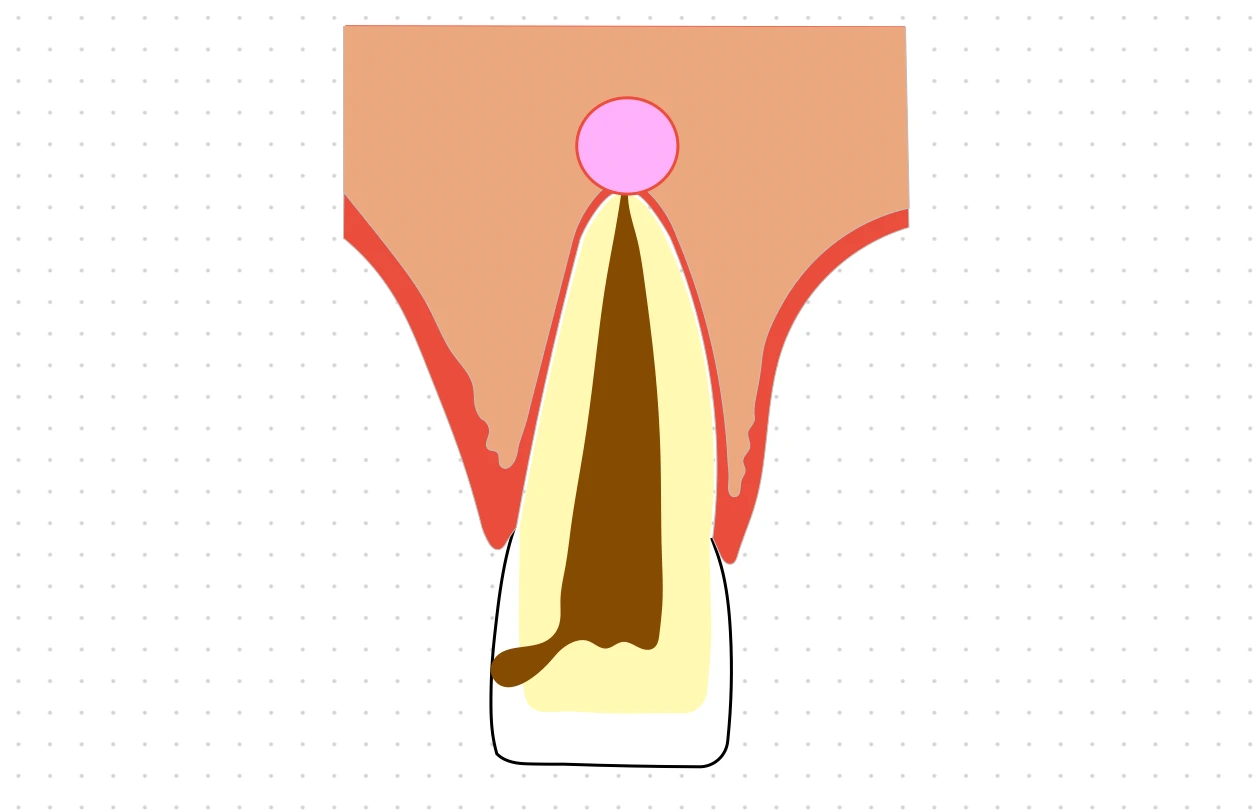
Periapcal cyst is an inflammatory odontogenic cyst that occurs in association with the root / apex of a non-vital tooth. It is classified as an inflammatory cyst, since, in most of cases it is associated with a periapical inflammatory response.
Etiology and Pathogenesis
- The usual etiology is an infected tooth, that leads to pulp necrosis. Other causes may include tooth fracture and improper restorations.
- The first line of defense to pulpal necrosis, is the formation of a granuloma in the periapical area.
- The granuloma provides a rich vascular supply, that stimulates the epithelial rests of Malassez.
- The epithelial rests of Malassez undergo proliferation and forms a large mass of cells,
- With continuous growth, the inner cells of the mass become deprived of nourishment. They die and autolyse, producing a central cavity.
- As the cavity forms, tissue fluid collects. The debris from dead epithelial cells and inflammatory exudate produces hydrostatic pressure that leads to expansion of the cyst.
- When the red cells in the cyst lumen or wall degenerate, their membranes release cholesterol, which crystallises and induces a foreign body inflammatory reaction with giant cells and macrophages.
- The other lipids from the membrane are taken up by macrophages that develop a foamy cytoplasm of engulfed fat droplets.
- Cluster of crystals and inflammatory cells form nodules in the wall ('mural nodules') that hang into the cyst cavity.
Clinical Findings
- Most common odontogenic cyst (60%).
- Asymptomatic (symptoms tend to present when the cyst becomes acutely inflamed).
- Associated tooth is seldom painful or sensitive to percussion.
- May develop into an abscess, due to acute exacerbation of the chronic inflammatory process.
Radiographic Features
- Well-circumscribed, round or oval radiolucency with a sharply defined outline.
- Condensed radiopaque corticated periphery may be found, if the growth is slow (usually more prominent in longstanding cysts).
Histologic Features
- Initially, the cyst is no more than a periapical granuloma containing a few strands of proliferating epithelium. Later, a well-organised thick cyst wall with epithelial lining and dense inflammatory infiltrate develops.
- The fibrous wall consists of collagenous connective tissue (abundant fibroblasts) with variable inflammatory infiltrate.
- Lymphocytes are generally the most prominent cells in the infiltrate, characterised by their darkly stained nucleus, which occupies most of the cytoplasm.
- The cystic wall also have abundant plasma cells, that are characterised by eccentric nucleus with cartwheel arrangement of the nuclear chromatin.
- The lining consists of non-keratinising stratified squamous epithelium of variable thickness. More inflamed cysts have a more hyperplastic epithelium that appears net-like, forming rings and arcades.
- The epithelial lining, many times, is discontinuous, frequently missing over areas of intense inflammation.
- Hyaline body or Rushton Body are often found in great numbers in the epithelium.
- The cystic lumen usually contains a fluid with low concentration of protein that stains palely eosinophilic.
- Long standing cysts typically have a thin flattened epithelial lining, a thick fibrous wall and less inflammatory infiltrate.
Differential Diagnosis
Any well-circumscribed unilocular radiolucency adjacent to the root of a tooth should be considered in the differential.
- Periapical cemento-osseous dysplasia
- Periapical cementoma (early stages) : The tooth is vital, mostly involves the incisors.
- Periapical granuloma : If the radiolucency is smaller than 1.5 cm, then it is most likely to be a granuloma. Cysts show a straw coloured fluid on aspiration.
- Periapical scar : Can be eliminated on the basis of history and location.
- Initial stage of odontogenic keratocyst, ameloblastoma and even lymphoma.
Treatment Options
- Extraction of the involved teeth and careful curettage of the periapical tissue : A residual cyst may develop, if the cystic sac is badly fragmented, leaving epithelial remnants, or if the cyst or granuloma is incompletely removed.
- Endodontic treatment with apicoectomy and curettage of the cystic lesion can also be considered.
Points to Note
-
Non-vital teeth mostly remain in an asymptomatic state, causing no more than a periapical granuloma.
-
A granuloma is a highly vascularised tissue containing a profuse infiltrate of immunologically competent cells, i.e, lymphocytes, macrophages and plasma cells.
-
The epithelial rests of Malassez present in the periapical region, are pluripotent in nature and can differentiate into any type of epithelium, under proper stimuli.
-
Hyaline body or Rushton Body : Tiny linear or arc-shaped bodies that appear amorphous in structure, eosinophilic in reaction and brittle in nature.
-
Residual cyst :
- Can be defined as a retained periapical cyst that develops after removal of the associated tooth and cyst.
- Appears as a well-circumscribed radiolucency located at the site of a previously extracted tooth.
- Treatment involves conservative surgical excision.
- The cyst does not recur, since the tooth associated with the pathogenesis of the cyst has been removed.
-
Bay Cyst : Periapical granuloma without cystic transformation, composed of islands of squamous epithelium.
-
Lateral radicular cyst : A radicular cyst that develops on the lateral side of a non-vital tooth root, at the opening of a lateral root canal, rather than at the apex.
-
Chair-side method for differentiating cysts and granuloma
- Using alkaline copper tartarate in cystic fluid aspirate.
- Cyst aspirate shows an intense albumin pattern, with definite pattern in globular zones on polyacrylamide gel electrophoresis.
- Granuloma aspirate shows only a faint-to-moderate pattern in the albumin zone.
References
- Shafer, Hine, Levy Shafer's Textbook of Oral Pathology (7th edition), Editors - R Rajendran, B Sivapathasundharam, Elsevier.
- Cawson's Essentials of Oral Pathology and Oral Medicine (9th Edition), E. W. Odell, Elsevier.
- Textbook of Oral Medicine (3rd edition), Anil Govindrao Ghom, Savita Anil Ghom (Lodam), Jaypee Brothers Medical Publishers (P) Ltd.
- Burket's Oral Medicine (13th edition), Michael Glick, Martin S. Greenberg, ,Peter B. Lockhart, Stephen J. Challacombe, Wiley Blackwell.
*This article is an excerpt from the above mentioned books and Medical Sutras does not make any ownership or affiliation claims.