Peptic ulcer disease is characterised by a burning epigastric pain, caused by a break in the mucosal lining of the stomach and/or duodenum. The break in the mucosal surface is more than 5 mm in size, with depth to the submucosa.
Gastroduodenal Mucosal Defense
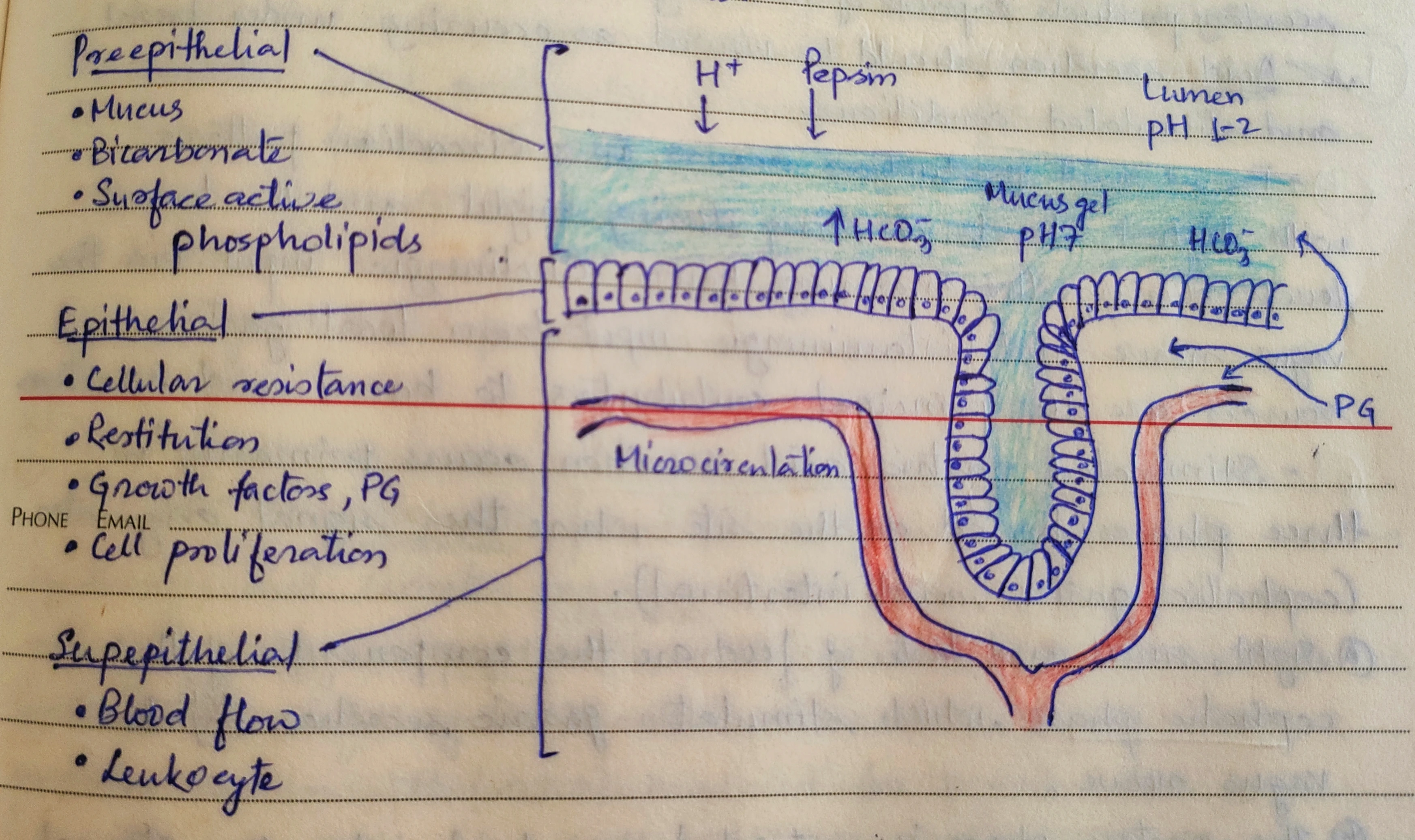
The gastric mucosa is under a constant attack by a host of noxious agents (acid, pepsin, bile salts, pancreatic enzymes, drugs and bacterias). However, it is protected by a three-level barrier composed of pre-epithelial, epithelial and sub-epithelial elements.
-
Pre-epithelial : Mucus, Bicarbonate, Surface active phospholipids.
-
Epithelial : Cellular resistance, Restitution, Growth factors, Prostaglandins, Cell proliferation.
-
Sub-epithelial : Blood flow, Leukocytes.
Etiology
-
H. pylori infection (accounts for the majority of cases).
-
NSAIDs.
-
Cigarette smoking
-
Genetic predisposition.
-
Psychological stress.
-
Dietary habit (eg. Consumption of beverages containing alcohol and caffeine).
-
Specific chronic disorders :
- Systemic mastocytosis.
- Chronic pulmonary disease.
- Chronic renal failure.
- Cirrhosis.
- Nephrolithiasis.
- Alpha-antitrypsin deficiency.
Clinical Features
History
-
Epigastric pain described as a burning or gnawing discomfort.
- Duodenal Ulcer : Pain typically occurs 90 minutes to 3 hours after a meal and is frequently relieved by antacids or food.
- Gastric Ulcer : Pain is precipitated by food, with nausea and vomiting being more common.
-
Variation in the abdominal pain and associated symptoms may indicate ulcer complication :
- Penetrating ulcer (pancreas) : Constant dyspepsia, not relieved by food or antacids or radiates to the back.
- Perforation : Sudden onset of severe generalised abdominal pain.
- Gastric outlet obstruction : Pain worsening with meals, nausea and vomiting of undigested food.
- Gastrointestinal Bleeding : Tarry stools or coffee ground emesis.
Physical Examination
- Epigastric tenderness is the most common finding.
- Dehydration (Secondary to vomiting or active g.i. blood loss) : Tachycardia and orthostasis.
- Perforation : Severely tender, board-like abdomen.
- Gastric outlet obstruction : Presence of succussion splash, indicating retained fluid in stomach.
Diagnostic Evaluation
Radiography (Barium study)
- Duodenal ulcer : Appears as a well-documented crater, most often seen in the bulb.
- Benign gastric ulcer : Appears as a discrete crater with radiating mucosal folds originating from the ulcer margins.
- Malignant gastric ulcer : Ulcers appears greater than 3 cm in size or associated with a mass.
Endoscopy
- Allows direct visualisation of the mucosa, photographic documentation of mucosal defect and tissue biopsy.
- Most sensitive and specific method to examine upper gastrointestinal tract.
Test for detection of H. pylori
- Invasive (Biopsy required) : Rapid urease, Histology, Culture.
- Non-invasive : Serology, Urease breath test, Stool antigen.
Complications
Gastro-intestinal bleeding
- Most common complication (around 15%).
- Higher incidence in elderly due to increased use of NSAIDs.
Perforation
- Second most common complication (6-7%).
- The contents of stomach escape into the peritoneal cavity leading to peritonitis.
Penetration
- Form of perforation, in which the ulcer bed tunnels into an adjacent organ.
- Duodenal ulcers : Tends to penetrate posteriorly into the pancreas, leading to pancreatitis.
- Gastric ulcers : Tend to penetrate into the left hepatic lobe.
Gastric outlet obstruction
- Least common complication (1-2%).
- Cardinal signs : Nausea, vomiting, abdominal distention.
- May occur secondary to ulcer-related inflammation and edema or a fixed, mechanical obstruction due to scar formation, in the peri-pyloric region.
Management
General Measures
- Avoid cigarette smoking and use of NSAIDs.
- Alcohol in moderation is not harmful and no special dietary advice is required.
Medications
-
Drugs that inhibit acid secretion :
- H2 antagonists : Ranitidine (150mg BD).
- Proton pump inhibitors : Pantoprazole (40mg OD), Rabeprazole (20mg OD).
-
Drugs that enhance mucosal defense and prokinetic agents :
- Colloidal bismuth (125mg 6 hourly).
- Misoprostol (200mg 6 hourly).
- Sucralfate (2g BD).
- Domperidone (10-20mg TDS).
Surgical Treatment
-
Emergency surgery is indicated in case of perforation and haemorrhage while elective surgery is indicated when there are complications such as gastric outflow obstruction and recurrent ulcer following gastric surgery.
-
In emergency situation, under-running the ulcer for bleeding or oversewing (patch repair) for perforation is recommended.
-
The treatment of choice for chronic non-healing gastric ulcer is partial gastrectomy, preferably with a Billroth I anastomosis.
-
Complications of gastric resection or vagotomy :
- Early satiety and vomiting.
- Bile reflux gastritis.
- Late Dumping Syndrome.
- Diarrhoea and maldigestion.
- Weight loss.
- Anemia.
- Metabolic bone disease.
- Gastric cancer.
Points to Note
-
Restitution : Restoration of a damaged region by migration of gastric epithelial cells bordering the site of injury.
-
Role of Prostaglandins :
- Regulates release of mucosal bicarbonate and mucus.
- Maintains the blood flow of the gastric mucosa and epithelial cell restitution.
-
Cigarette smoking appears to decrease healing rate, impair response to therapy and increase ulcer related complications.
-
Succussion splash (Gastric splash) : Sloshing sound, heard during sudden movement of the patient on abdominal auscultation. It reflects the presence of gas and fluid in an obstructed organ, as in gastric outlet obstruction.
-
A large number of patients suggestive of ulcer have non-ulcer dyspepsia, hence, in healthy individuals with age less than 45 years, empirical therapy is recommended before starting any diagnostic evaluation.
-
Radiographic studies that shows a gastric ulcer must be followed by endoscopy and biopsy, since gastric ulcers (around 8%) that appear benign by appearance are found malignant on endoscopy and biopsy.
-
Billroth I anastomosis : The ulcer and ulcer-bearing area of the stomach are resected.
References
-
Harrison's Principles of Internal Medicine (17th edition), Fauci, Braunwald, Jasper, Hauser, Longo, Jameson, Loscalzo, The McGraw-Hill Companies.
-
The image used in the cover is licensed under the Creative Commons Attribution-Share Alike 4.0 International license.
- Description : Gastric Ulcer.
- Source : Own work.
- Author : BruceBlaus.
*This article is an excerpt from the above mentioned book and Medical Sutras does not make any ownership or affiliation claims.