The olfactory nerve, or 1st cranial nerve is a purely sensory nerve, that belongs to the special visceral afferent column, and, carries the sense of smell from nasal cavity.
Anatomy & Pathway
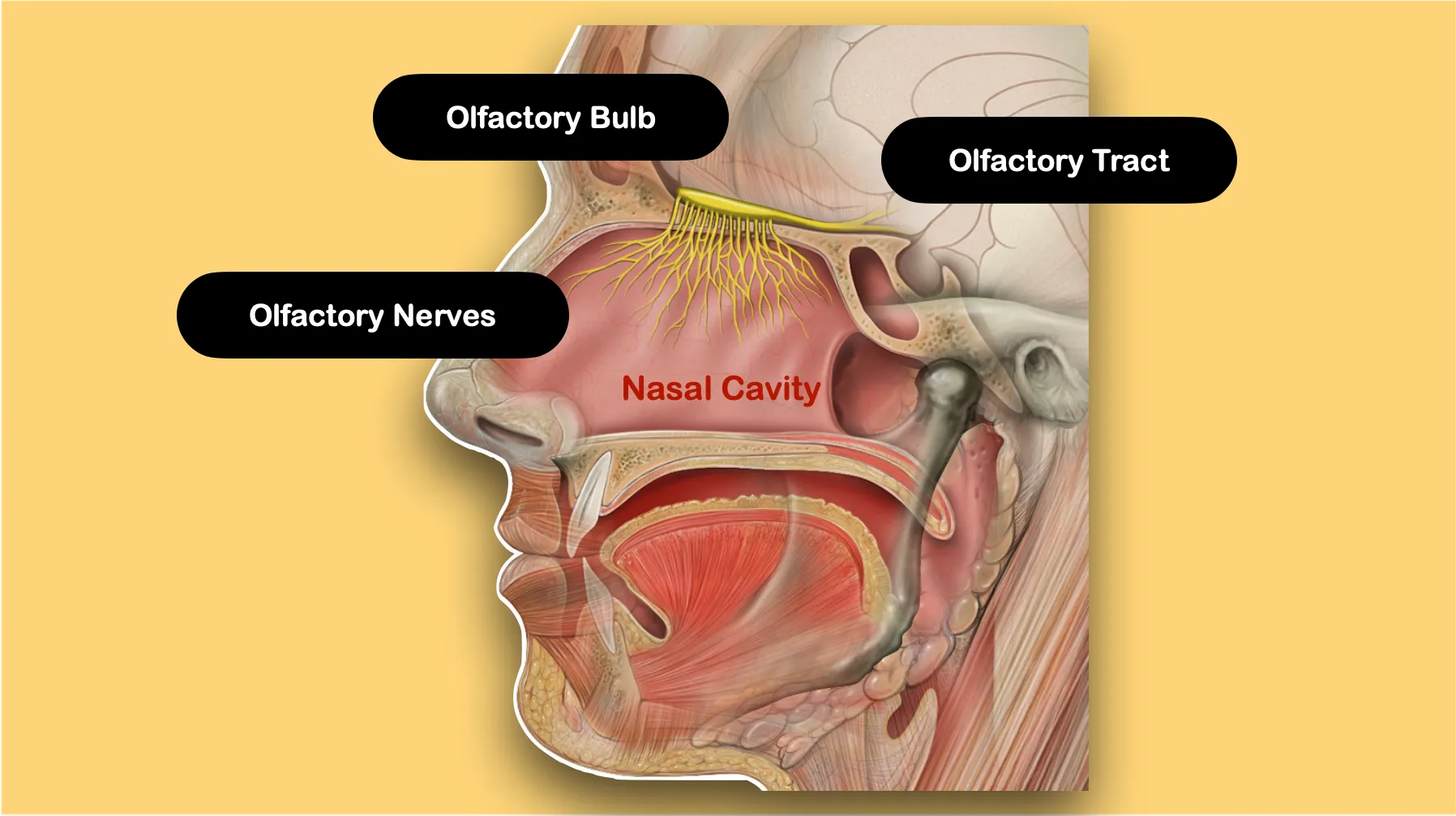
- Each olfactory nerve consists of about 20 bundles of incredibly thin unmyelinated axons that originate from the olfactory receptor cells (about 0.2 μm in diameter).
- The olfactory receptor cells are specialized sensory receptor cells (about 6 million in number) nestled among the supporting mucosal cells (olfactory epithelium) in the roof of the nasal cavity on protuberances called concha.
- The olfactory nerve formed by the coalescence of the olfactory receptor cells, ascend about 30 mm from the nasal cavity through the cribriform plate of the ethmoid and enter the anterior cranial fossa.
- In the cranial cavity, olfactory nerve axons synapse in an ovoid extrusion of the cerebral cortex that rests on the cribriform plate called the olfactory bulb (about 8 mm2 in size).
- The olfactory bulb consist of cells arranged in six concentric layers. Each olfactory neuron only synapses with one or two olfactory bulb cells so that the receptor-specific odorant response is preserved.
- The primary output neurons of the olfactory bulb project directly via the olfactory tract to brain structures (the primary olfactory cortex).
Clinical Significance
The disorders of olfactions can be manifested in several forms:
- Anosmia: Complete loss of the ability to detect odors.
- Partial anosmia: Loss of the ability to detect some, but not all, odors.
- Hyposmia/Microsmia: Decreased sensitivity to olfactory stimuli.
- Hyperosmia: Increased sensitivity to olfactory stimuli.
- Dysosmia/Parosmia: Distortion of olfactory perception.
- Cacosmia: When the order is perceived as fetid (extremely unpleasant).
- Phantosmia: Perception of odor when no true olfactory stimulus is present, such as olfactory hallucinations.
- Olfactory agnosia: Inability to recognize an odor that can be perceived.
Etiology
- Conductive or transport impairment: Resulting from mechanical obstruction of the nasal passage as in chronic nasal inflammation.
- Sensorineural impairment: Due to damage to the olfactory epithelium as might occur after a viral infection.
- Central olfactory neural impairment: Involves central nervous system damage such as when tumors compress the olfactory tract (e.g., meningiomas), and neurodegenerative disorders.
Post-traumatic olfactory dysfunction: Involves all three mechanisms:
- Sinus or nasal tract disruption,
- Shearing of olfactory nerve fibers at the cribriform plate, and
- Localized hemorrhage/contusion within the olfactory bulb and primary olfactory cortex
Isolated congenital anosmia: A rare condition inherited in an autosomal dominant fashion and characterized by a lifelong inability to smell, with no associated congenital structural or metabolic abnormalities.
Kallmann syndrome: A form of hypogonadotropic hypogonadism that is differentiated by the additional and unique symptoms of anosmia.
- It occurs as a result of impaired development of the olfactory system and disrupted embryonic migration of GnRH-synthesizing neurons from the olfactory epithelium to the hypothalamus.
- The failure to develop proper early olfactory neuron projections from the olfactory placode to the olfactory bulb results in aplasia or hypoplasia of the olfactory bulbs that are visible on MRI.
Testing of Olfactory Nerve
- Using odorants with characteristic smell such as menthol oil, lavender oil, coffee, ammonia, clove, vinegar, pepper, and turpentine.
- Smell Identification test: Consists of four booklets, each containing 10 “scratch & sniff” odorants.
- Electrophysiological test: Evaluate either electrical activity at the surface of the olfactory epithelium (electro-olfactogram), or, integrated electrical activity on the scalp in response to odors (i.e., odor-event recorded potentials).
Points to Note
- It is the shortest cranial nerve, with the simplest anatomy of any of the cranial nerves.
- Embryologically, the olfactory nerve is a derivative of the forebrain and is therefore considered a component of the central nervous system.
- The olfactory nerve is not myelinated by Schwann cells but rather is ensheathed by olfactory ensheathing glia.
- It can regenerate if damaged, provided the supporting layer of cells is preserved.
- It is capable of repenetrating the cribriform plate and form new connections with the olfactory bulb when damaged.
- It projects directly to the brain (olfactory bulb) without any intervening synapse. This allows a precise relationship between odorants and their recognition, however, it also forms a primary route for exposure of brain to viruses, bacterias and other airborne toxins.
- Humans have approximately 350 functional types of olfactory receptors, each responding to a few specific odorants.
- Not all sensations that we associate with smell are in fact truly conveyed by the olfactory nerve. The trigeminal nerve has sensory branches in the mouth and nose that respond to sensations such as warmth, coolness, pungency, and irritation.
- Assessing olfactory symptoms in cases like stroke is clinically unhelpful because an isolated unilateral stroke in the primary olfactory cortex will not result in significant olfactory symptoms. The primary olfactory cortex in each hemisphere receives input bilaterally, from both olfactory bulbs.
References
-
[](https://amzn.to/3Ixnict) Textbook of Anatomy Head, Neck, and Brain (Volume III), Vishram Singh
[](https://amzn.to/3IazzTM) The Clinical Anatomy of the Cranial Nerves, : The Nerves of "On Old Olympus Towering Top"
-
Helwany M, Bordoni B. Neuroanatomy, Cranial Nerve 1 (Olfactory) [Updated 2023 Aug 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK556051/
-
The image used is licensed under the Creative Commons Attribution 2.5 Generic license. (Author: Patrick J. Lynch, medical illustrator. Source: Wikimedia Commons.)
*This article is an excerpt from the above mentioned sources and Medical Sutras does not make any ownership or affiliation claims.