Odontogenic keratocyst is a developmental odontogenic cyst characterised by a thick layered (8-10 cell layers) parakeratinised epithelium with palisaded, polarised basal cell layer (often described as picket-fence or tombstone appearance).
In 2005, WHO classified the lesion as a tumor and named it Keratocystic Odontogenic Tumor (KOT). However, in 2016, it re-considered the decision and reversed the classification to Odontogenic Keratocyst (OKC).
The reasons to consider the lesion as cystic neoplasm includes :
- Aggressive clinical behaviour.
- High recurrence rate.
- High mitotic count of basal and para-basal layers.
- Association with PTCH (patched), a tumor suppressor gene and gp38 positivity (seen in cells with neoplastic potential, suggestive of altered gene expression of the epithelial cells).
Origin
- OKC develops from the rests of odontogenic epithelium that remain in the alveolus after tooth development, probably Cell Rests of Serres (remnants of dental lamina epithelium entrapped within the gingiva).
Pathogenesis
- The pathogenesis of OKC involves a two hit mechanism, with allelic loss at chromosome 9q, which results in inactivation of the tumor suppressor gene (PTCH gene).
- The inactivation of tumor suppressor gene (in one-third cases) or any other genetic faults in the signalling pathways results in high proliferative activity of the cystic epithelial lining.
- This leads to enlargement of the cyst by growth of the epithelial lining (rather than internal pressure), and hence, the lining becomes folded as growth of the wall exceeds that of the cavity containing the cyst.
- Extensions of the lining penetrate the wall, forming small daughter cysts that enlarge to produce a multi-locular lesion.
- The cyst wall produces bone-resorbing factors that resorbs the surrounding medullary bone, allowing the cyst to enlarge slowly along the medullary cavity.
- *Two-hit mechanism : It is the process by which a tumor suppressor gene is inactivated. The first hit involves mutation in one allele that has no phenotypic effect, while the second hit refers to loss of the other allele (Loss of Heterozygosity), which leads to the dysregulation of oncoproteinss cyclin D1 and p53.
Clinical Features
- Usually asymptomatic, until the bone is expanded or become infected.
- Age : Peak incidence around 20-30 years.
- Gender : Male predilection.
- Location : More common in mandible (majority occur in ramus-third molar area).
- Symptoms associated with secondary infection : Pain, soft-tissue swelling, expansion of bone and drainage.
- Neurologic manifestations such as paresthesia of lip or teeth may occur in case of nerve involvement.
- The chances of secondary infection in maxillary cyst are more due to its vicinity to the maxillary sinus.
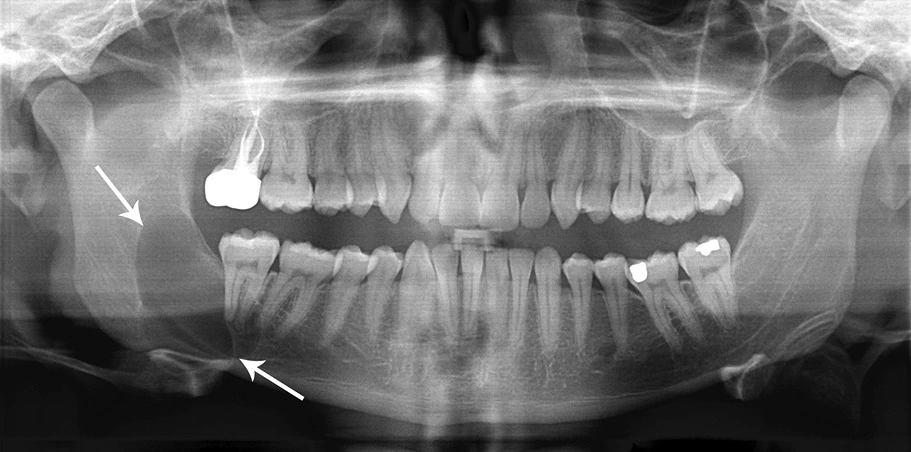
Radiographic Findings
- Appear as well-defined radiolucent areas, mostly unilocular with smooth borders, but multi-locular cysts are also observed.
- Usually the radiolucency is hazy due to keratin filled cavity and is surrounded by thin sclerotic margin due to reactive osteocytes.
- There is extensive spread of the lesion along the medullary cavity with minimal bone expansion, tooth displacement, root resorption or displacement of inferior alveolar nerve. This does not occur until the whole medulla is involved.
Histologic Features
Epithelial lining
- Consists of stratified squamous epithelium with a corrugated thinly para-keratinised surface and a palisaded basal layer of columnar cells that shows reverse polarity and resembles pre-ameloblast (indicating odontogenic origin).
- No rete ridges are present, hence, the epithelium often sloughs from the connective tissue (94% cases).
- However, in the presence of intense inflammation, the adjacent epithelium loses its keratinised surface, may thicken and develop rete ridges or may ulcerate.
Connective tissue
- The connective tissue wall often shows scattered islands of odontogenic epithelium similar to the lining epithelium. These represent the ends of folds of the lining epithelium and forms small satellite or daughter cysts, which can enlarge to become separate locules in a multi-locular cyst.
Cystic lumen
- May be filled with a thin straw colored fluid or with a thicker creamy material.
- Sometimes the lumen contains large amount of keratin and cholesterol and hyaline bodies may also be found (at sites of inflammation).
Differential Diagnosis
Multi-locular radiolucency must be differentiated from :
- Ameloblastoma.
- Central giant cell granuloma.
- Odontogenic myxoma.
- Calcifying epithelial odontogenic tumor(early lesions prior to calcification).
Multiple odontogenic keratocysts can be found in :
- Gorlin Goltz syndrome.
- Marfan syndrome.
- Ehler's Danlos syndrome.
- Noonan's syndrome.
Treatment Modalities
Treatment depends mainly on the extent of the cyst and degree of multilocularity.
-
Unilocular and small multi-locular cyst can be treated conservatively by enucleation and vigorous curettage (to remove every fragment of cyst lining).
-
Marsupialisation followed by enucleation : Recommended for large multi-locular cyst, as it is easier to enucleate the residual cyst (there is reduction in size with ingrowth of oral epithelium into the cavity, replacing keratinised epithelium with non-keratinising stratified squamous epithelium). Also, morbidity is considerably less compared to radical surgery and the displaced teeth often regain an upright position.
-
Resection and reconstruction with a bone graft : Indicated for most extensive cysts that cannot be managed by above method.
-
Treatment of cyst cavity with Carnoy's solution : Additional precautionary measure, wherein the Carnoy's solution is applied either before enucleation to kill and toughen the lining for removal or after curettage (to the bony walls) to destroy residual epithelial cells.
- Carnoy's solution kills and denatures tissue to a depth of apprx. 1-2mm, enough to kill the full thickness of the wall.
- It is a caustic solution, containing ferric chloride, alcohol, chloroform and highly concentrated acetic acid and must be used with care near vital structures such as inferior alveolar nerve.
- Also, the inclusion of chloroform makes it controversial to use.
Recurrence
Odontogenic keratocyst have a very high rate of recurrence. Possible reasons include :
- Thin, fragile epithelial lining with complex outline : Very difficult to remove completely.
- Extension of the cyst into the medullary spaces.
- Presence of satellite or daughter cysts.
- Intrinsic growth potential in the epithelial lining, leading to more rapid proliferation of the keratocyst.
*Since recurrence may be long delayed, follow-up with annual radiographs is essential for at least five years after surgery.
Orthokeratinised Odontogenic Cyst
- Here, stratified squamous epithelium produces orthokeratin.
- It is less common (10%) than the parakeratinised type (83%), with considerably less aggressive behaviour.
Basal Cell Nevus Syndrome
-
Also called Gorlin's / Gorlin-Goltz syndrome, Bifid Rib Syndrome, Jaw Cyst-Basal cell nevus, Cutaneomandibular polyoncosis.
-
Inherited as an autosomal dominant trait.
-
Caused by mutation of the PTCH1 gene on chromosome 9q22.3-31.
-
Clinical Features :
- Cutaneous anomalies : Basal cell carcinoma, Pitting of the soles and palms, Palmar and plantar keratosis, and Dermal calcinosis.
- Dental anomalies : Odontogenic keratocysts, Mild mandibular prognathism.
- Skeletal anomalies : Rib abnormalities (often bifid), Vertebral anomalies, Brachymetacarpalism.
- Ophthalmologic abnormalities : Hypertelorism with wide nasal bridge, Dystopia canthorum, Congenital blindness, Internal strabismus.
- Neurologic anomalies : Mental retardation, Dural calcification, Agenesis of corpus callosum, Congenital hydrocephalus.
- Sexual abnormalities : Hypogonadism in males and ovarian tumors.
References
-
Burket's Oral Medicine, 13th Edition, Michael Glick, Martin S. Greenberg, ,Peter B. Lockhart, Stephen J. Challacombe, Wiley Blackwell.
-
Shafer, Hine, Levy Shafer's Textbook of Oral Pathology (7th Edition), Editors - R Rajendran, B Sivapathasundharam, Elsevier.
-
Cawson's Essentials of Oral Pathology and Oral Medicine, 9th Edition, EW Odell, Elsevier.
-
Textbook of Oral Pathology, 2nd Edition, Anil Govindrao Ghom, Shubhangi Mhaske (Jedhe) - Jaypee Brothers Medical Publishers (P) Ltd.
-
The image used is licensed under the Creative Commons Attribution 3.0 Unported license.
- Description : Classic look to a keratocyctic odontogenic tumor in the right mandible in the place of a former wisdom tooth. Unicystic lesion growing along the bone. Lesion was seen by oral surgeon on routine panoramic radiography without any symptoms.
- Author : Coronation Dental Specialty Group.
*This article is an excerpt from the above mentioned book and Medical Sutras does not make any ownership or affiliation claims.