It is the third cranial nerve, that is purely motor and responsible for the movement and accommodation of eye.
Functional Components
General Somatic Efferent Fibres
-
Arise from the somatic component of oculomotor nucleus, also called somatic motor nucleus.
-
Supplies all extraocular muscles, except, (A3 SO4 LR6)
- Superior oblique: Supplied by 4th cranial nerve.
- Lateral rectus: Supplied by 6th cranial nerve.
General Visceral Efferent Fibres
- Arise from the parasympathetic component of oculomotor nucleus, also called the Edinger-Westphal nucleus.
- These are preganglionic parasympathetic fibres and relay in the ciliary ganglion.
- The postganglionic parasympathetic fibres arise from ganglion and supply the sphincter pupillae and ciliaris muscles.
Anatomy & Pathway
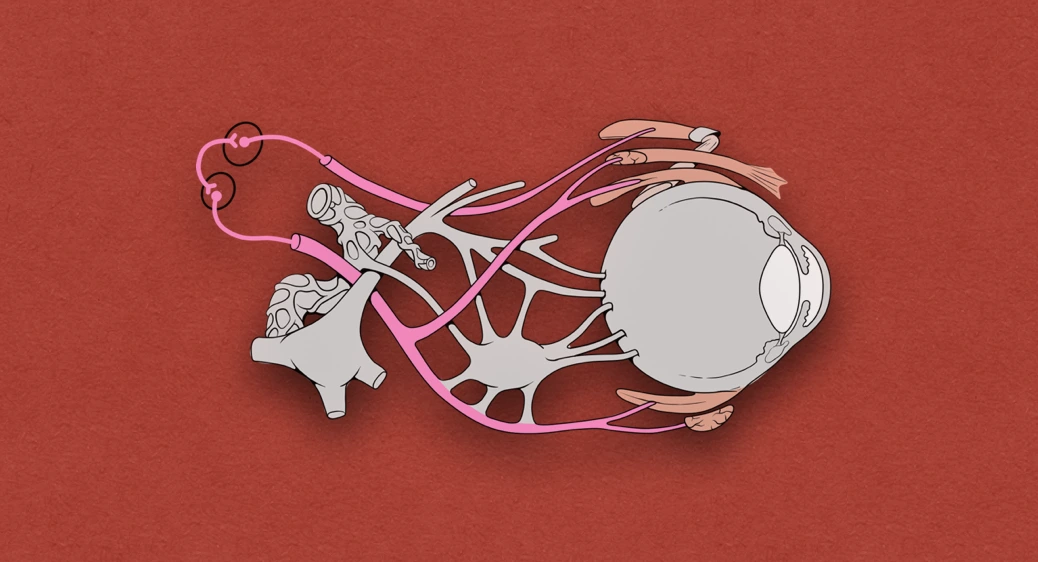
- Starts from the oculomotor sulcus on the medial aspect of the cerebral peduncle of the midbrain and appears in the interpeduncular fossa.
- Runs forward and laterally between the posterior cerebral and superior cerebellar arteries, and lateral to the posterior communicating artery.
- It passes through the tentorial notch of tentorium cerebelli to reach the middle cranial fossa.
- In the middle cranial fossa, the nerve pierces the dura mater in the oculomotor triangle lying in between the free and attached margins of tentorium cerebelli in the roof of the cavernous sinus, and enters the lateral wall of the cavernous sinus.
- In the anterior part of the cavernous sinus, it divides into upper and lower divisions, which enters the orbit through the superior orbital fissure within the common tendinous ring.
- Upper division of optic nerve (smaller): Passes above the optic nerve on the inferior surface of superior rectus and then passes through the superior rectus to supply the levator palpebrae superioris.
- Inferior division of optic nerve (larger): Passes below the optic nerve and immediately gives three branches which supply the medial rectus, inferior rectus, and inferior oblique muscles.
- The nerve to inferior oblique gives motor root (parasympathetic root) to the ciliary ganglion located in the posterior part of the orbit.
- The postganglionic fibres from this ganglion run through short ciliary nerves and supply the sphincter pupillae and ciliaris muscles.
Clinical Significance
Damage of oculomotor nerve may occur due to compression by:
- Aneurysm of the posterior communicating artery.
- Aneurysm of the internal carotid artery.
- Transtentorial uncal herniation.
The clinical features in case of damage to oculomotor nerve are:
- Ptosis: Drooping of the upper eyelid, due to paralysis of the levator palpebrae superioris.
- Lateral strabismus: Lateral squint due to paralysis of the medial rectus and consequent unopposed action of lateral rectus.
- Dilated and fixed pupil: Due to paralysis of the sphincter pupillae and consequent unopposed action of dilator pupillae.
- Loss of accommodation: Due to paralysis of the medial rectus, sphincter pupillae and ciliaris muscles.
- Diplopia: Double vision on looking medially, inferiorly and superiorly, due to paralysis of the medial rectus, inferior rectus and inferior oblique muscles.
- Proptosis: Prominence of eyeball due to relaxation of the muscles of eyeball.
References
| [](https://amzn.to/3Ixnict)
Textbook of Anatomy Head, Neck, and Brain (Volume III), Vishram Singh |
- The image used is licensed under the Creative Commons Attribution 2.5 Generic license. (Author: Patrick J. Lynch, medical illustrator. Source: Wikimedia Commons.)
*This article is an excerpt from the above mentioned sources and Medical Sutras does not make any ownership or affiliation claims.