Mouth breathing is the habitual respiration through mouth instead of nose. It can be classified as:
- Anatomic: Have short upper lip or proclined upper anterior teeth, that does not permit complete closure without undue effort.
- Obstructive/Pathological: Have an an increased resistance to, or a complete obstruction of, the normal air flow through the nasal passages.
- Habitual: Continually breathes through the mouth by force of habit, although the abnormal obstruction has been removed.
Etiologic factors
- Enlarged nasal turbinates, adenoids or tonsils.
- Deviated nasal septum and other nasopharyngeal deformities.
- Allergic rhinitis.
- Nasal polyps.
- Abnormally short upper lip.
- Obstruction in the bronchial tree or larynx.
- Obstructive sleep apnea syndrome.
- Genetically predisposed children (Ectomorphic children having a genetic type of tapering face and a nasopharynx are prone to nasal obstruction).
- Thumb sucking or similar habits.
Clinical Features
Systemic Findings
- Pigeon-chest appearance (Pectus Carinatum): It refers to a chest wall deformity in which the sternum protrudes anteriorly. Mouth breathing is not as deep as nasal breathing as there is no nasal resistance. The diaphragm and intercostal muscles do not perform much work to create negative pressure to promote airflow into the lungs. This leads to insufficient expansion of lungs and interferes with the development of the chest resulting in postural defects.
- Low-grade oesophagitis: There is a lack in oesophageal lubrication, as the oropharynx is dry and mucus collected, is often expectorated.
- Abnormal blood gas constituents Mouth breathers have 20% more carbon dioxide and 20% less oxygen in the blood.
- No purification of the inspired air.

Image Credit: Tolson411 (Source: Wikimedia Commons, License: Creative Commons Attribution-Share Alike 3.0 Unported)
Adenoid Facies
The term was coined by CV Thomas (1872) to describe the dentofacial changes associated with chronic nasal airway obstruction.
- Long, narrow face that is often expressionless.
- Narrow nose with slit-like external nares (due to disuse atrophy of the lateral cartilages, caused by long standing nasal airway obstruction).
- Incompetent lip posture: Flaccid lips with short upper lip and fuller lower lip.
- Gummy smile (excessive appearance of upper anterior teeth).
- V-shaped, high palatal vault (as the buccal segments of maxilla are collapsed).
- Gingivitis in the anterior maxillary arch: Gingiva is hyperplastic, with classic rolled margin and enlarged interdental papilla.
Dental Findings
- Retroclined upper and lower incisors.
- Posterior crossbite.
- Tendency towards an open bite, with flaring of incisors and decrease in overbite.
- Narrow palatal and cranial widths.
Cephalometric Findings
- Increased facial height.
- Increased mandibular plane angle.
- Retrognathic maxilla and mandible.
Other Findings
- Nasal tone in voice (speech).
- Otitis media.
- Decreased sense of smell and taste.
- Altered muscle activities (eg. lower activity of palatoglossus and levator palatine).
Clinical Examination
Study patient's breathing (without informing)
- Nasal breathers: Lips touching lightly during relaxed breathing.
- Mouth breathers: Keep their lips apart.
Ask patient to close the lips & take a deep breath
- Nasal breather: Usually dilates the nostrils (external nares) due to good reflex control of the alar muscles.
- Mouth breathers: Do not appreciably change the shape and size of the external nares and occasionally contracts the nasal orifices while inspiring.
Mirror Test
- A double sided mirror is held between the nose and mouth.
- Nasal breather: Fogging on the nasal side of the mirror.
- Mouth breather: Fogging on oral side.
Massler's Butterfly Test/Cotton Test
- A small wisp of cotton (butterfly shaped) is placed below the nostrils.
- Nasal breathing: The cotton fibres flutter down.
- This test can also be used to determine unilateral nasal blockage.
Water Holding Test
- The patient is asked to fill the mouth with water and retain it for a period of time.
- Mouth breathing: Inability to hold the water (keep mouth closed) for more than 2 minutes.
Inductive Plethysmography (Rhinomanometry)
- A rhinomanometer is used to measure air flow through the nasal passage and nasal resistance (Healthy children : 0.36 + 0.21 Pa/cm3/s, decreases with age).
- A high value of nasal resistance signifies nasal obstruction and mouth breathing.
Cephalometry
- Helps to establish amount of nasopharyngeal space, size of adenoids and to the skeletal patterns of the patient.
- Jaraback Ratio (used to assess vertical or horizontal growth pattern): Posterior facial height/Anterior facial height x 100.
Treatment
Mouth breathing should be treated during the mixed dentition period to prevent or correct any adverse effects on the occlusion.
The management involves:
- Elimination of cause.
- Prevention of habit.
- Correction of malocclusion.
- Symptomatic treatment.
Elimination of Cause
- Nasal or pharyngeal obstruction: Removal of nasal or pharyngeal obstruction by surgery or medication should.
- If a respiratory allergy is present, it should be brought under control.
- Narrow, constricted maxillary arches : Rapid maxillary expansion.
Prevention of Habit
Prevention or interception of mouth breathing habit can be achieved through
- Exercises: If there is no pathological cause, the patient should be instructed for breathing and lip exercises.
- Oral Screen/Vestibular Screen/Oral shield
Breathing Exercise
- Done in the morning and night.
- Deep breathing exercises are done with deep inhalation through the nose with arms raised sideways.
- After a short period, the arms are dropped to the sides and the air is exhaled through the mouth.
Lip Exercises
- The child is instructed to extend the upper lip, behind the maxillary incisors. This exercise should be done 15-30 minutes a day for a period of 4-5 months. when the child has a short upper lip. If the maxillary incisors are protruded, the lower. lip can be used to augment the upper lip exercise. The upper lip is first extruded into the previously described position, then, the vermillion border of the lower lip is placed against the outside of the extruded upper lip and pressed as hard as possible against the upper lip.
- Playing a wind instrument such as flute.
- Hold a celluloid strip, metal disk, sheet of paper or piece of card (1 x 11/2") between the lips : Necessitate the lip being closed and makes the child conscious of their opening if the object drops.
- Button pull exercise : The patient is asked to place a button of one and half inch diameter (with a thread passed through) behind the lip and then, pull the thread while restricting it from being pulled out by using lip pressure.
- Tug of war exercise : This involves two buttons, with one placed behind the lips while the other is held by another person to pull the thread.
Maxillothorax Myotherapy (advocated by Macaray in 1960)
- Expanding exercises used in conjunction with the Macaray activator.
- Macaray activator: A stable aluminium activator incorporated at the angle of the mouth, with horizontal hooks to which expanding rubber bands are attached.
- The mouth breathers holds the activator in the mouth and at the same time with the left and right arms alternatively carries out 10 exercises thrice daily.
- The child stands with his back against the wall, rises and lowers on his toes in time with the expander exercises holding the lips tight together and carries out a lightly forced breathing technique in front of an open window.
Oral Screen (Vestibular screen/Oral shield)
- Is a thin rubber membrane either cut or cast to fit in the labial vestibule (over the labial and buccal surfaces of the teeth and gums).
- It prevents the ingress of air through the mouth and directs contraction of lips against the anterior teeth,
- Reduction in anterior open bite is obtained after treatment for 3-6 months.
- During initial phase, windows are placed on the oral screen, so as not to completely block the airway passage.
- Should not be used if the child has naso-respiratory distress or nasal obstruction.
Correction of Malocclusion (Mechanical / Myofunctional appliances)
- Oral Shield appliance: Class I skeletal and dental malocclusion and anterior spacing.
- Monobloc activator: Class II Div I without crowding (age 5-9 years)
- Interceptive methods such as Chin cap: Class III malocclusion.
Symptomatic Treatment
The gingiva of mouth breathers should be restored to normal health by
- coating the gingiva with petroleum jelly,
- by applying preventive dentistry methods and
- by clinically correcting periodontal defects that have occurred due to the habit.
References
-
Orthodontics Diagnosis and Management of Malocclusion and Dentofacial Deformities (3rd edition), Om Prakash Kharbanda, Elsevier India (2020).
-
Textbook of Orthodontics (2nd Edition), Gurkeerat Singh, Jaypee Brothers Medical Publishers (P) Ltd.
-
The image used is licensed under Creative Commons Attribution-Share Alike International 4.0 license.
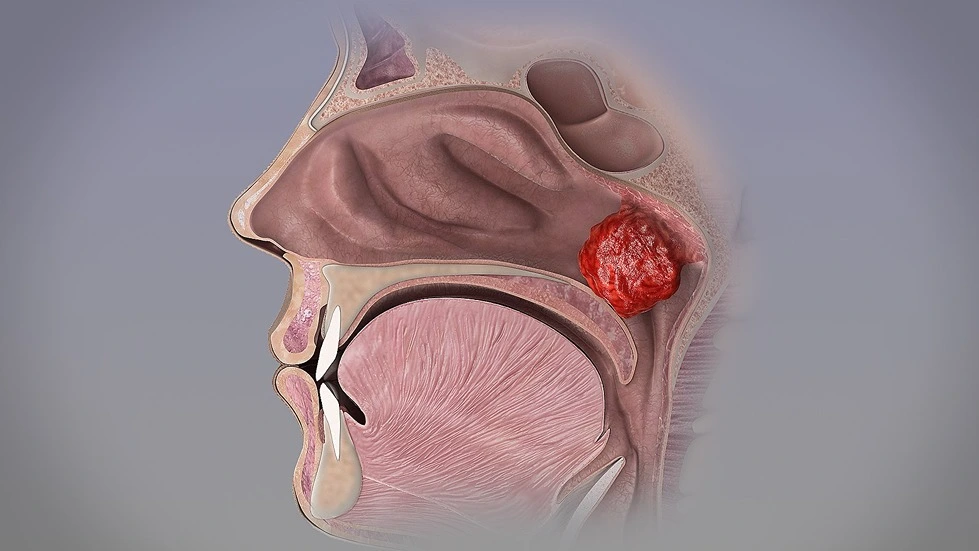
- Description : Adenoids become large enough to completely block the airflow through the nasal passages.
- Author : www.scientificanimations.com
- Source : http://www.scientificanimations.com/wiki-images/.
*This article is an excerpt from the above mentioned books and Medical Sutras does not make any ownership or affiliation claims.