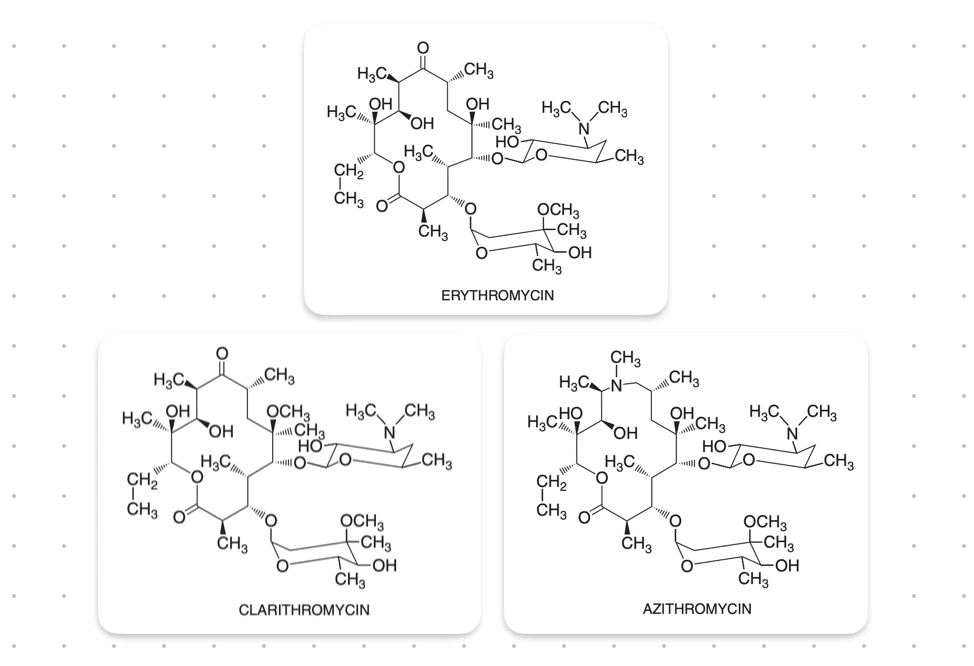
Macrolides are characterised by a macrocyclic lactone ring, usually containing 14 or 16 atoms (erythromycin and clarithromycin - 14 and azithromycin - 15), to which one or more deoxy sugars are attached.
Clarithromycin and Azithromycin, both are derived from erythromycin. Clarithromycin by addition of a methyl group, while Azithromycin by addition of methyl-substituted nitrogen in the lactone ring.
Mechanism of Action
- Macrolides are bacteriostatic agents (cidal in some cases), that are most active against aerobic gram-positive cocci and bacilli.
- They inhibit protein synthesis by binding reversibly to 50S ribosomal RNA near the peptidyltransferase center.
- Erythromycin interferes with the translocation step, wherein a newly synthesised peptidyl tRNA molecule fails to move from the acceptor(A) site on the ribosome to the peptidyl donor site. This makes the acceptor site unavailable for next aminoacyl tRNA attachment, resulting in the premature termination of the peptide chain.
Mechanism of Resistance
- Drug efflux by an active pump mechanism (most common in cocci).
- Ribosomal protection by a plasmid encoded methylase enzyme that alters the ribosomal target and decrease drug binding (important in gram-positive bacteria).
- Macrolide hydrolysis by esterases produced by Enterobacteriaceae.
- Chromosomal mutations that alter a 50S ribosomal protein (found in B. subtilis, Campylobacter spp., Mycobacteria and gram-positive cocci).
- Cross-resistance is found among macrolides and also with Clindamycin and Chloramphenicol (due to proximity of ribosomal binding sites).
Pharmacokinetics
Erythromycin
-
Absorption :
- Oral absorption is incomplete but adequate.
- Food interferes with absorption.
- Inactivated by gastric acid.
- Administered as enteric-coated tablets that dissolve in the duodenum or as an ester e.g., stearate, estolate and ethylsuccinate (less affected by food with improved acid stability).
-
Distribution :
- Diffuses rapidly into the intracellular fluids (does not cross blood-brain barrier).
- Protein binding is ~70-80% for erythromycin base and even higher for the estolate.
- Crosses the placenta and concentrations in fetal plasma are ~5-20% of those in maternal circulation.
- Concentration in breast milk are 50% of those in serum.
-
Elimination :
- The antibiotic is concentrated in the liver and is excreted in the bile (only 2-5% of orally administered, 12-15% after IV is excreted in active form in the urine).
- Dose reduction is usually not required in renal insufficiency.
- Half-life : ~1.5 hours.
Clarithromycin
-
Absorption :
- Rapidly absorbed after oral administration.
- Hepatic first pass metabolism reduces bioavailability to ~50%.
- May be given with or without food (extended-release form should be administered with food to improve bioavailability).
-
Distribution :
- High intracellular concentrations throughout the body.
- Tissue concentrations, incl. in the middle ear, generally exceed serum concentrations.
-
Elimination :
- Metabolised in the liver to several metabolites.
- Half-life : 3-7 hrs (active metabolite 14-hydroxyclarithromycin : 5-9 hrs).
- Metabolism is saturable, resulting in nonlinear pharmacokinetics and longer half-lives after larger doses.
- 20-40% is excreted unchanged in urine.
- Dose reduction is recommended for patients with creatinine clearance less than 30 ml/min.
Azithromycin
-
Absorption :
- Absorbed rapidly and well tolerated.
- Should not be given with food as it reduces bioavailability.
-
Distribution :
- Distributed widely throughout the body, except to the brain and CSF.
- Extensive tissue concentrations (exceeding serum concentrations by 10 to 100-fold), with high drug concentrations within cells (including phagocytes).
- Slowly released from the tissues, hence, allows once-daily dosing and shortening of the duration of treatment in many cases.
-
Elimination :
- Undergoes some hepatic metabolism to inactive metabolites.
- Biliary excretion is the major route of elimination.
- Only 12% excreted unchanged in the urine.
- Half-life 40-68 hours (due to extensive tissue sequestration and binding).
Dosages
Erythromycin
- Adults : 1-2 g/day, in divided doses, given every 6 hours.
- Children : 30-50 mg/kg/day, divided into four portions, dose may be doubled for severe infections.
- IV administration (Erythromycin lactobionate) : Reserved for severe infections, such as legionellosis. Usual dose : 0.5-1 g every 6 hours.
Clarithromycin
- Adults and children older than 12 years : 250 mg twice daily (500 mg twice daily in serious infections such as pneumonia or H. influenzae).
- Children (younger than 12 years) : 7.5 mg/kg twice daily
Azithromycin
- Adult : 250-500 mg/day.
- Children : 5-10 mg/kg.
Indications
-
Atypical pneumonia caused by Mycoplasma pneumoniae.
-
Whooping cough (Pertussis) : Erythromycin estolate (40mg/kg/day, max 1g/day) is the drug of choice for treatment and post-exposure prophylaxis of household members and close contacts. Has little influence once the paroxysmal stage is reached.
-
Legionnaires' Disease : Azithromycin is the first-line drug (due to excellent activity, superior tissue concentration, once-daily dosing and better tolerability) : 500 mg daily IV or oral for 10-14 days.
-
Chlamydial infections : All macrolides are effective.
- Azithromycin is recommended for patients with uncomplicated urethral, endocervical, rectal or epididymal infections (because of ease of compliance).
- Erythromycin base : Recommended for chlamydial urogenital infections during pregnancy (500 mg 4 times daily for 7 days), chlamydial pneumonia of infancy and ophthalmia neonatorum (50mg/kg/day in 4 divided doses for 10-14 days).
-
H. pylori infection : Clarithromycin (100mg) in combination with Lansoprazole (30mg) and Amoxicillin (1g) twice daily. Clarithromycin (500mg) in combination with Omeprazole (20mg) and Amoxicillin (1g) twice daily for 10-14 days effeective for treatment of peptic ulcer disease caused by H.pylori.
-
Chancroid and PPNG urethritis : Azithromycin 1g single dose is highly curative.
Other uses of Azithromycin
-
Community-acquired pneumonia, Pharyngitis, Skin and skin-structure infections : Loading dose 500mg on the first day, followed by 250 mg/day for additional days.
-
Prophylaxis of M. avium-intracellulare infection in AIDS patients : Azithromycin 500 mg daily in combination with other agents for treatment or 1200mg once weekly for primary prevention.
-
Treatment of STDs, especially during pregnancy when tetracyclines are contraindicated.
-
Indication and dosage in children :
- Acute otitis media and pneumonia : 10 mg/kg on the first day (maximum 500 mg) and 5 mg/kg (maximum 250 mg/day) on day 2-5.
- Tonsillitis or phrayngitis : 12 mg/kg/day, upto 500 mg total, for 5 days.
Second-line therapy
- Diphtheria : Erythromycin 250 mg 4 times daily for 7 days is very effective for acute infections or for eradicating the carrier state.
- Streptococcal infections : Valuable alternatives in patients with serious allergy to penicillin, but macrolide resistance is increasing.
- Campylobacter infections : Erythromycin remains useful for treatment of Campylobacter gastroenteritis in children. (Fluoroquinolones are preferred in adults).
- Tetanus : Erythromycin (500 mg orally every 6 hours for 10 days) may be given to eradicate C. tetani in patients allergic to penicillin.
- Leptospirosis : erythromycin 250 mg 6 hourly for 7 days in patients allergic to penicillins.
- Prophylaxis of recurrences if rheumatic fever in individuals allergic to penicillin.
Adverse Effects
- Serious side effects are rare.
- Allergic reactions include fever, eosinophilia and rash, resolves after the therapy is stopped.
- Cholestatic hepatitis : Most striking side effect, caused primarily by erythromycin estolate (may be due to hypersensitivity reaction to the estolate ester).
- Gastrointestinal effects (Epigastric distress) : Anorexia, nausea, vomiting and diarrhoea.
Drug Interactions
- Erythromycin and clarithromycin inhibit CYP3A4 and cause significant drug interactions. Potentials the effects of carbamazepine, glucocorticoids, cyclosporine, digoxin, ergot alkaloids, theophylline, triazolam, valproate and coumadin.
- Azithromycin lacks these drug interactions, since it has a 15-member (instead of 14-member) lactone ring.
Points to Note
- The activity of macrolides is enhanced in alkaline medium, since higher pH favours the nonionised (penetrable) form of the drug.
- Food ideally should not be taken concurrently with erythromycin base or the stearate formulations but is acceptable with erythromycin estolate or erythromycin ethylsuccinate.
- Azithromycin should be taken 1 hour before or 2 hours after meal, since food decreases bioavailability.
- Bordetella pertussis has reported resistance to Erythromycin and nasopharyngeal cultures should be obtained if pertussis does not improve with erythromycin therapy.
- Penicillin-resistant Staphylococci and Streptococci shows resistance to erythromycin also.
- Erythromycin has been studied as prophylaxis against endocarditis during dental procedures in individuals with valvular heart disease who are unable to tolerate amoxicillin, but clindamycin which is better tolerated has largely replaced it.
References
- Laurence L. Brunton - Goodman & Gilman's Manual of Pharmacology and Therapeutics-McGraw-Hill Medical (2008).
- Essentials of Medical Pharmacology (8th Edition), K.D. Tripathi -Jaypee Brothers Medical Publishers (P) Ltd.
- Basic and Clinical Pharmacology (15th Edition), Bertram G. Katzung, Todd W. Vanderah, McGraw Hill Lange.
*This article is an excerpt from the above mentioned books and Medical Sutras does not make any ownership or affiliation claims.