The International Classification of Diseases to Dentistry and Stomatology grouped injuries to the periodontal tissues as under:
- N 503.20: Concussion.
- N 503.20: Subluxation (Loosening).
- N 503.20: Extrusive luxation (Peripheral dislocation, Partial avulsion).
- N 503.20: Lateral luxation.
- N 503.21: Intrusive luxation (Central dislocation).
- N 503.22: Avulsion (Exarticulation).
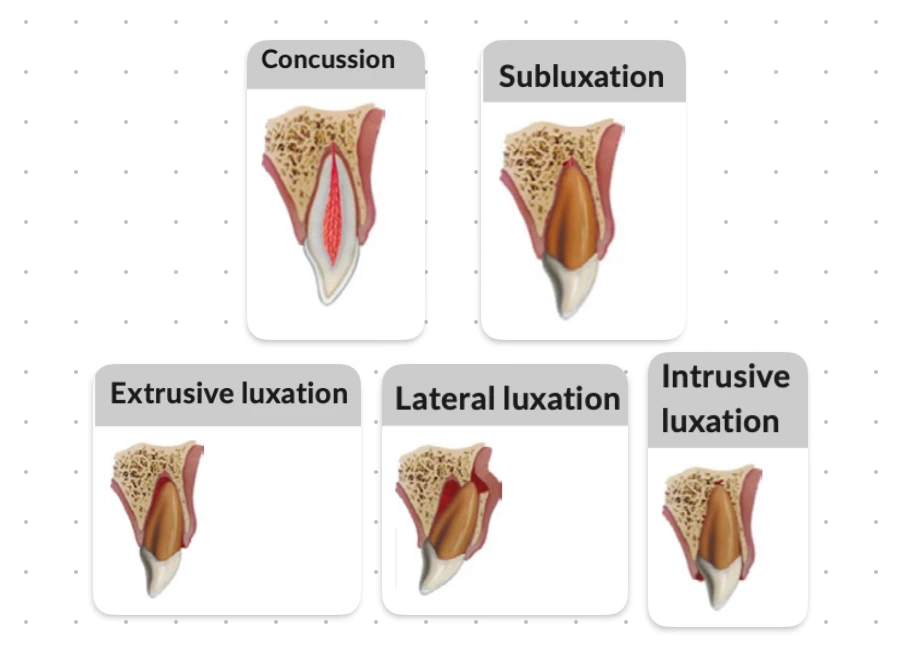
Concussion
An injury to the tooth-supporting structures, wherein the tooth shows marked reaction to percussion, but without any abnormal loosening or displacement.
Clinical Findings
- Normal mobility.
- The tooth is tender to touch and percussion.
- Tooth will likely respond to pulp sensibility testing.
Radiographic Findings
-
No radiographic abnormalities.
-
Recommended radiographs:
- One parallel IOPA radiograph.
- Additional radiographs are recommended if signs or symptoms of other potential injuries are present.
Treatment
- No treatment is required.
- Monitor pulp condition for at least one year, but preferably longer.
- Follow up: At 4 weeks and 1 year.
Favourable Outcomes
- Asymptomatic.
- Positive response to pulp sensibility testing; however, a false negative response is possible for several months. Endodontic treatment should not be started solely on the basis of no response to pulp sensibility testing.
- Continued root development in immature teeth.
- Intact lamina dura.
Unfavourable Outcomes
- Symptomatic.
- Pulp necrosis and infection.
- Apical periodontitis.
- No further root development in immature teeth.
Subluxation
There is an abnormal loosening of the tooth due to injury of the tooth-supporting structures, but no demonstrable displacement of the tooth.
Clinical Findings
- The tooth is tender to touch or light tapping.
- Tooth has increased mobility but is not displaced.
- Bleeding from the gingival crevice may be present.
- Tooth may not respond to pulp sensibility testing initially indicating transient pulp damage.
Radiographic Findings
-
Radiographic appearance is usually normal.
-
Recommended radiographs:
- One parallel IOPA radiograph.
- Two additional radiographs of the tooth taken with different vertical and/or horizontal angulations.
- Occlusal radiograph.
Treatment
-
Normally, no treatment is needed.
-
A passive and flexible splint is recommended (to stabilise the tooth for upto 2 weeks) :
- When there is excessive mobility or tenderness when biting on the tooth.
- If several teeth are traumatised or subluxated.
-
Monitor the pulp condition for at least one year, but preferably longer.
-
Follow up: At 2 weeks (splint removal), 12 weeks, 6 months and 1 year.
Favourable Outcomes
- Asymptomatic.
- Positive response to pulp sensibility testing; however, a false negative response is possible for several months. Endodontic treatment should not be started solely on the basis of no response to pulp sensitibility testing.
- Continued root development in immature teeth.
- Intact lamina dura.
Unfavourable Outcomes
- Symptomatic.
- Pulp necrosis and infection.
- Apical periodontitis.
- No further root development in immature teeth.
- External inflammatory (infection-related) resorption: If this type of resorption develops, RCT should be initiated immediately, with the use of calcium hydroxide as an intracanal medicament. Alternatively, corticosteroid / antibiotic medicament can be used initially, which is then followed by calcium hydroxide.
Extrusion (Extrusive Luxation)
There is partial displacement of the tooth out of its socket, in an incisal or axial direction.
Clinical Findings
- The tooth appears elongated (incisally).
- Tooth has increased mobility.
- Likely to have no response to pulp sensibility tests.
Radiographic Findings
-
Increased PDL space both apically and laterally.
-
Tooth will not be seated in its socket and will appear elongated incisally.
-
Recommended radiographs:
- One IOPA radiograph.
- Two additional radiographs of the tooth taken with different vertical and/ or horizontal angulations
- Occlusal radiograph.
Treatment
- Reposition the tooth by gently pushing it back into the tooth socket under local anaesthesia.
- Stabilise the tooth for 2 weeks using a passive and flexible splint. If there is breakdown or fracture of the marginal bone, splint for an additional 4 weeks.
- Monitor the pulp condition with pulp sensibility tests.
- If the mature tooth does not respond to pulp vitality tests within 2-3 weeks after repositioning, endodontic treatment should be undertaken before evidence of root resorption appears.
- The prognosis for severely loosened primary tooth is poor and frequently, it remains mobile and undergo rapid resorption.
Follow up
- At 2 weeks (splint removal), 4 weeks, 8 weeks, 12 weeks, 6 months, 1 year and then yearly for at least 5 years.
- Patients and parents (where relevant) should be informed to watch for any unfavourable outcomes and the report to the clinic if they observe any.
- Where unfavourable outcomes are identified, treatment is often required.
Favourable Outcomes
- Asymptomatic.
- Clinical and radiographic signs of normal or healed periodontium.
- Positive response to pulp sensibility testing; however, a false negative response is possible for several months. Endodontic treatment should not be started solely on the basis of no response to pulp sensibility testing.
- No marginal bone loss.
- Continued root development in immature tooth.
Unfavourable Outcomes
- Symptomatic.
- Pulp necrosis and infection.
- Apical periodontitis.
- Breakdown of marginal bone.
- External inflammatory (infection-related) resorption: If this type of resorption develops, RCT should be initiated immediately, with the use of calcium hydroxide as an intracanal medicament. Alternatively, corticosteroid/ antibiotic medicament can be used initially, which is then followed by calcium hydroxide.
Lateral Luxation
There is displacement of the tooth in a lateral direction or any direction other than long axis of the tooth. It is usually associated with fracture or compression of the alveolar socket wall or facial cortical bone.
Clinical Findings
- Tooth is displaced, usually in a palatal/lingual or labial direction.
- Associated fracture of the alveolar bone.
- Tooth is frequently immobile, as the apex of the root is "locked in" by the bone fracture.
- High metallic (ankylotic) sound on percussion.
- Likely to have no response to pulp sensibility tests.
Radiographic Findings
-
Widened PDL space, best seen on radiographs taken with horizontal angle shifts or occlusal exposures.
-
Recommended radiographs:
- One parallel IOPA radiograph.
- Two additional radiographs of the tooth taken with different vertical and/or horizontal angulations.
- Occlusal radiograph.
Treatment
-
Apply local anaesthesia.
-
Palpate the gingiva to feel the apex of the tooth and then disengage it from its locked position
-
Gently reposition the tooth to its normal position: Use one finger to push downwards over the apical end of the tooth, then use another finger or thumb to push the tooth back into its socket.
-
Stabilise the tooth for 4 weeks using a passive and flexible splint. If there is breakdown/fracture of the marginal bone or alveolar socket wall, additional splinting time may be required.
-
Monitor the pulp condition with pulp sensibility tests at the follow-up appointments.
-
At about 2 weeks post-injury, make an endodontic evaluation.
-
Tooth with incomplete root formation:
- Spontaneous revascularisation may occur.
- If the pulp becomes necrotic and there are signs of inflammatory (infection-related) external resorption, RCT should be started as soon as possible.
- Endodontic procedures suitable for immature teeth should be used.
-
Tooth with complete root formation:
- The pulp will likely become necrotic.
- Root canal treatment should be started, using corticosteroid-antibiotic or calcium hydroxide as an intracanal medicament to prevent the development of inflammatory (infection-related) external resorption.
Follow up
- At 2 weeks, 4 weeks (splint removal), 8 weeks, 12 weeks, 6 month, 1 year. Then, yearly for at least 5 years.
- Patients or parents should be informed to watch for any unfavourable outcomes and the need to return to clinic if they observe any.
- Where unfavourable outcomes are identified, treatment is often required.
Favourable Outcomes
- Asymptomatic.
- Clinical and radiographic signs of normal or healed periodontium.
- Positive response to pulp sensibility testing; however, a false negative response is possible for several months. Endodontic treatment should not be started solely on the basis of no response to pulp sensibility testing.
- Marginal bone height corresponds to that seen radiographically after repositioning.
- Continued root development in immature teeth.
Unfavourable Outcomes
- Symptomatic.
- Breakdown of marginal bone.
- Pulp necrosis and infection.
- Apical periodontitis.
- Ankylosis.
- External replacement resorption.
- External inflammatory (infection-related) resorption: If this type of resorption develops, root canal treatment should be initiated immediately, with the use of calcium hydroxide as an intracanal medicament. Alternatively, corticosteroid/ antibiotic medicament can be used initially, which is then followed by calcium hydroxide.
Intrusion (Intrusive Luxation)
There is displacement of the tooth in an apical direction (along the long axis of the tooth) into the alveolar bone.
Clinical Findings
- Tooth is displaced apically into the alveolar bone.
- Tooth is immobile.
- Associated with fracture of the alveolar bone.
- High metallic (ankylotic) sound on percussion.
- Likely to have no response to pulp sensibility tests.
Radiographic Findings
-
The PDL space may not be visible for all or part of the root (especially apically).
-
The cemento-enamel junction is located more apically in the intruded tooth than in adjacent non-injured teeth.
-
Recommended radiographs:
- One parallel IOPA.
- Two additional radiographs of the tooth taken with different vertical and/or horizontal angulations.
- Occlusal radiographs.
Treatment
-
Teeth with incomplete root formation (Immature teeth):
- Spontaneous re-eruption : Allow re-eruption without intervention for all intruded teeth independent of the degree of intrusion.
- If there is no re-eruption within 4 weeks : Initiate orthodontic repositioning.
- Monitor the pulp condition.
- In teeth with incomplete root formation, spontaneous pulp revascularisation may occur. However, if it is noted that the pulp becomes necrotic or infected or that there are signs of inflammatory (infection-related) external resorption at follow-up appointments, RCT is indicated and should be started as soon as possible when the position of the tooth allows. Endodontic procedures suitable for immature teeth should be used.
-
Teeth with complete root formation (Mature teeth):
- Intrusion less than 3 mm : Allow re-eruption without intervention. If no eruption within 8 weeks, reposition surgically and splint for 4 weeks with a passive and flexible splint. Alternatively, reposition orthodontically before ankylosis develops.
- Intrusion 3-7 mm : Reposition surgically (preferably) or orthodontically.
- Intrusion more than 7mm : Reposition surgically.
- In teeth with complete root formation, the pulp almost always becomes necrotic. RCT should be started at 2 weeks or as soon as the position of the tooth allows, using a corticosteroid-antibiotic or calcium hydroxide intracanal medicament. The purpose of this treatment is to prevent development of inflammatory (infection-related) external resorption.
Follow up
- At 2 weeks, 4 weeks (Splint removal) , 8 weeks, 12 weeks, 6 months and 1 year.
- Then, yearly for at least 5 years.
- Patients and parents should be informed to watch for any unfavourable outcomes and the need to return to clinic if they observe any.
- Where unfavourable outcomes are identified, treatment is often required.
Favourable Outcomes
- Asymptomatic.
- Tooth in place or is re-erupting.
- Intact lamina dura.
- Positive response to pulp sensibility testing; however, a false negative response is possible for several months. Endodontic treatment should not be started solely on the basis of no response to pulp sensibility testing.
- No signs of root resorption.
- Continued root development in immature tooth.
Unfavourable Outcomes
- Symptomatic.
- Tooth locked in place or ankylotic tone to percussion.
- Pulp necrosis and infection.
- Apical periodontitis.
- Ankylosis.
- External replacement resorption.
- External inflammatory (infection-related) resorption: If this type of resorption develops, RCT should be initially, initiated immediately, with the use of calcium hydroxide as an intracanal medicament. Alternatively, corticosteroid/ antibiotic medicament can be used initially, which is then followed by calcium hydroxide.
References
- Bourguignon C, Cohenca N, Lauridsen E, et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations. Dent Traumatol. 2020;36:314–330. https://doi.org/10.1111/edt.12578.
- McDonald and Avery's Dentistry for the Child and Adolescent (11th Edition) -Mosby (2021). https://amzn.to/3vZh9m7
*This article is an excerpt from the above mentioned books and Medical Sutras does not make any ownership or affiliation claims.