Keratoacanthoma is a relatively common low-grade malignant lesion that originates in the pilosebaceous gland and resembles squamous cell carcinoma, clinically and pathologically.
The definite cause remains unclear, but, some of the etiologic factors include,
- Sunlight.
- Exposure to pitch and tar.
- Trauma.
- Human papilloma virus (Type 9,11,13,16,18,24,25,33,37, and 57).
- Genetic factors : Chromosomal aberrations such as gains on 8q, 1p and 9p with deletions on 3p, 9p, 19p and 19q.
- Immunocompromised status.
Clinical findings
Age : Reported in all groups, incidence increases with age.
Gender : More common (2:1) in men than women.
Ethnicity : Less common in darker skinned individuals.
Site : Mostly occur on sun-exposed areas, common sites include face, neck and dorsum of the upper extremities.
Presentation
Appears as an elevated (dome-shaped) umbilicated or crateriform lesion measuring 1-1.5 cm in diameter, with a depressed central core or plug.
- Growth phase : It begins as firm, round, skin-colored or reddish papules that are typically solitary and develops to full size over a period of 4-8 weeks. It progress to dome-shaped nodules with a smooth shiny surface and a central crateriform ulceration or keratin plug (may project like a horn).
- Stationary phase : It persists as a static lesion for another 4-8 weeks.
- Involution phase : Involves spontaneous regression over the next 6-8 weeks by expulsion of the keratin core and resorption of the mass.
- Often painful with regional lymphadenopathy.
Differential diagnosis
- Actinic keratosis.
- Molluscum contagiosum.
- Muir-Torre syndrome.
- Squamous cell carcinoma.
- Verrucous carcinoma.
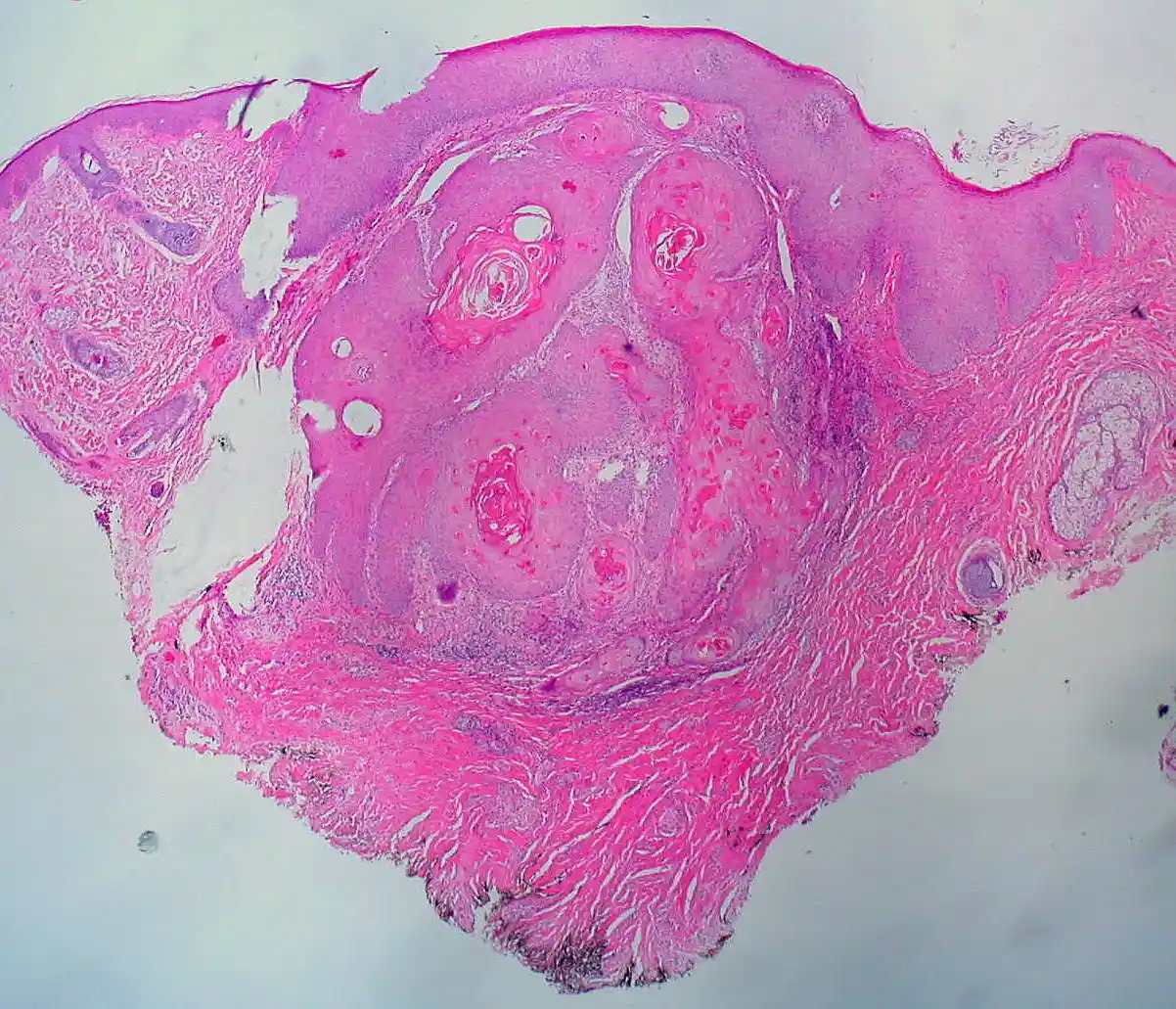
Histologic Findings
It consists of hyperplastic squamous epithelium growing into the underlying connective tissue.
- Surface is covered by thick layer of parakeratin or orthokeratin with central plugging.
- Islands of epithelium often appear to be invading at the deep margins of the tumor.
- Pseudocarcinomatous infiltration : Smooth, well-demarcated front, not extending beyond the level of the sweat glands.
- Connective tissue shows chronic inflammatory cell infiltration.
- Abrupt change in normal epithelium to hyperplastic acanthotic epithelium is seen at the margins.
Treatment
Keratoacanthoma is usually treated by surgical excision, if not resolved spontaneously.
- Prognosis is excellent following surgery, however, recurrent lesions may require more aggressive treatment.
- The patients should be followed for the development of new primary skin cancers, esp. squamous cell carcinoma.
Points to Note
- Other names : Self-healing carcinoma, Pseudocarcinoma, Keratocarcinoma, Molluscum sebaceum.
- Muir-Torre syndrome : Autosomal dominant phenotypic variant of hereditary non-polyposis colorectal cancer, characterised by sebaceous neoplasms of the skin and visceral malignancies (colonic carcinoma being the most common).
References
-
Shafer, Hine, Levy Shafer's Textbook of Oral Pathology (7th Edition), Editors - R Rajendran, B Sivapathasundharam, Elsevier.
-
Textbook of Oral Pathology, 2nd Edition, Anil Govindrao Ghom, Shubhangi Mhaske (Jedhe) - Jaypee Brothers Medical Publishers (P) Ltd.
-
The image used is licensed under the Creative Commons Attribution-Share Alike 2.0 Generic license.
- Source : https://www.flickr.com/photos/euthman/2197016313/.
- Author : Ed Uthman, MD.
*This article is an excerpt from the above mentioned book and Medical Sutras does not make any ownership or affiliation claims.