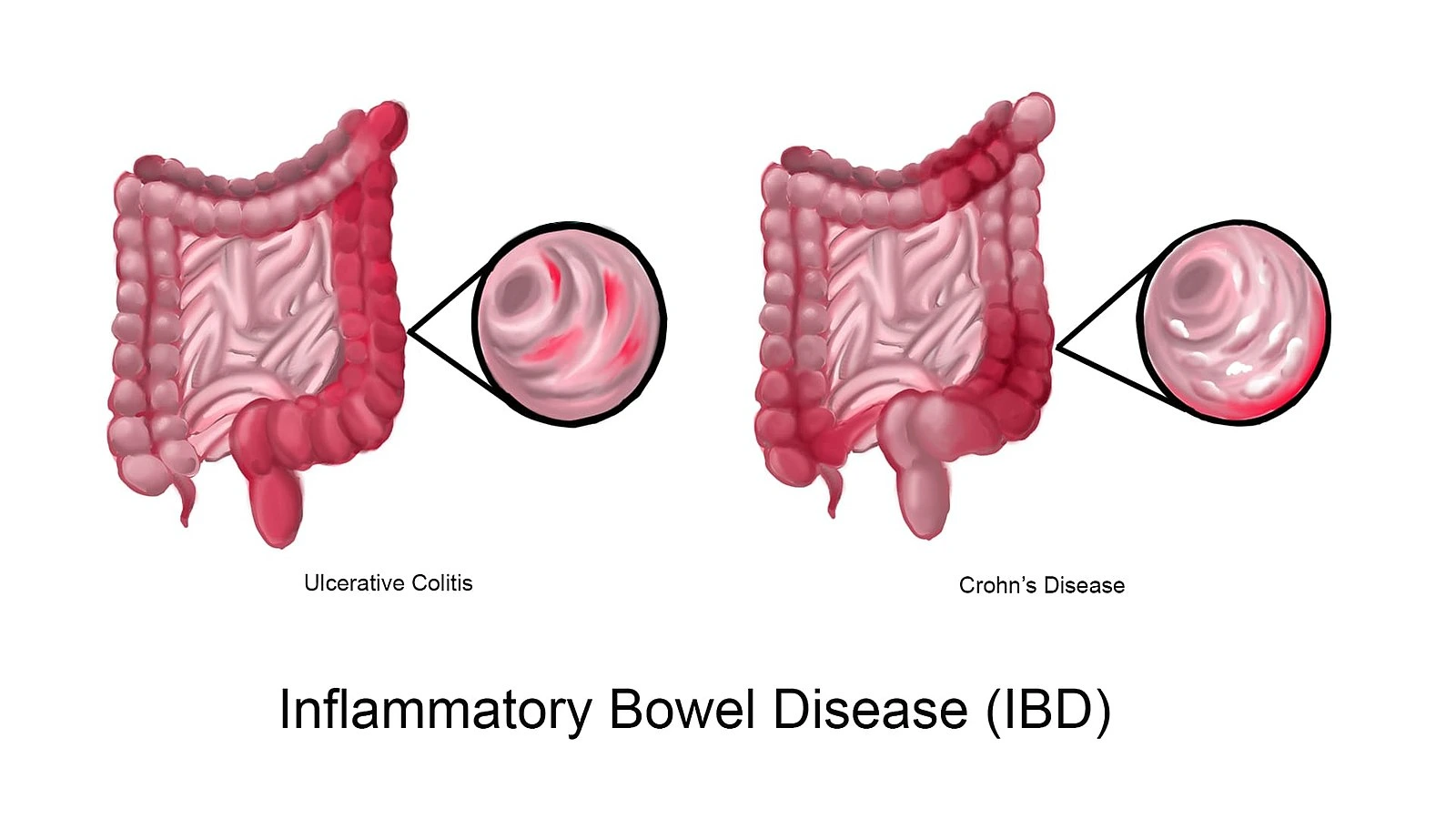
Inflammatory bowel disease (IBD) is a chronic idiopathic inflammatory disease of the gastrointestinal tract. The two major types of IBD are Ulcerative Colitis (UC) and Crohn's Disease (CD).
Epidemiology
-
Age of Onset : Peak incidence is in 20-40 years and 70-90 years.
-
Not gender specific.
-
Ethnicity : Greatest incidence is among white and Jewish people.
-
Urban areas and high socioeconomic classes have a higher prevalence rate.
-
IBD in children can be grouped as :
- Early onset IBD : Patients less than 10 years old.
- Very early onset IBD : Patients less than 6 years old.
- Infantile IBD : Patients below 2 years old.
Risk factors
- First degree relative with IBD (strongest risk factor).
- Smoking (important in caucasian populations).
- Oral contraceptive use : Increased risk of CD, while in UC, the increased risk is limited to women with a history of smoking.
- Infectious gastroenteritis with pathogens (e.g., Salmonella, Shigella, Campylobacter spp., Clostridium difficle) increase risk by 2-3 fold.
- Diet high in animal protein, sugars, sweets, oils, fish and shellfish, and dietary fat (esp. omega-6 fatty acids) and low in omega-3 fatty acids.
Protective factors
- Breast feeding : May protect against development of IBD.
- Previous appendectomy with confirmed appendicitis particularly at a young age has a protective effect on the development of UC. (Modestly associated with CD).
- Vitamin D : Protective effect on the risk of CD has been reported.
Etiology and Pathogenesis
The etiology and pathogenesis of IBD have not been defined.
- Under normal conditions, there is homeostasis between the three major host compartments i.e., commensal microbiota, intestinal epithelial cells (epithelial cells that line the interior of the intestines) and immune cells, and they function together as an integrated "supraorganism".
- A consensus hypothesis is that specific environmental factors (e.g., smoking, antibiotics, enteropathogens) and genetic factors (in a susceptible host) affects the functioning of the commensal microbiota, intestinal epithelial cells and immune cells. This results in disruption of homeostasis and culminate in chronic state of dysregulated inflammation i.e., IBD.
- Any causative external agent has not been identified yet. Hence, IBD is considered as an inappropriate immune response to the endogenous (autochthonus) commensal microbiota within the intestines, with or without involvement of autoimmunity.
Genetic considerations
The majority of cases of IBD are multigenic or polygenic in origin, that suggests a syndromic nature of the disease, giving rise to multiple clinical subgroup other than UC and CD. A monogenic etiology may also be possible in a small subset of adult patients with IBD.
Points supporting role of genetics include:
- Concordance in identical twins.
- Familial origin in at least 10% of afflicted individuals, consistent with an inherited basis for the disease.
- More than 60 different gene defects have been identified in patients with VEOIBD.
- Occurrence in the context of several genetic syndromes
- Development of severe, refractory IBD in early life in association with single-gene defects that affect the immune system.
Primary genetic disorders associate with IBD:
- Turner's syndrome.
- Hermansky-Pudlak syndrome.
- Wiskott-Aldrich syndrome.
- Glycogen storage disease type B1
- Immune dysregulation polyendrocinopathy, enteropathy X-linked (IPEX)
- Early onset IBD.
Commensal microbiota
-
Humans are born with sterile gut and acquire their commensal microbiota initially from the mother during birth and subsequently from environmental sources.
-
The composition and function of the intestinal microbiota is maintained by the host (e.g., immune and epithelial responses), environmental (e.g., diet and antibiotics), and likely genetic (e.g., NOD2) factors. In turn, the microbiota through its structural components and metabolic activity influences the epithelial and immune function of the host.
-
In some cases, absence of bacteria may exacerbate the activation of certain elements of intestinal immune system, resulting in severe colitis.
-
The commensal microbiota in patients with IBD is different from that of normal individuals :
- There is presence of microorganisms that drive disease (e.g., Proteobacteria such as enteroinvasive and adherent E. coli) and to which the immune response is directed.
- Loss of microorganisms that hinder inflammation (e.g., Firmicutes such as Faecalibacterium prausnitzii).
-
CD may show improvement with agents that alter the intestinal microbiota such as metronidazole, ciprofloxacin and elemental diets.
Defective immune regulation
- There are very powerful pathways within the immune system (e.g., T regulatory cells that express the FoxP3 transcription factor and suppress inflammation) , that restrain the gut from full immunologic response to the commensal microbiota and dietary antigens.
- In normal host, full activation of intestinal lymphoid tissues occurs in response to infections or other environmental stimuli, however, there is rapid dampening of the immune response and tissue repair.
- In IBD, the suppression of this response is altered, leading to uncontrolled inflammation.
Differential Diagnosis
Infectious causes
- Bacterial : Salmonella, Shigella, Toxigenic E. coli, Campylobacter, Cl. difficle, Gonorrhea, etc.
- Mycobacterial : M. tuberculosis, M. avium.
- Parasitic : Amebiasis, Isospora, Hookworm, Stringyloides.
- Viral : Cytomegalovirus, Herpes simplex, HIV.
- Fungal : Histoplasmosis, Candida, Aspergillus.
Noninfectious causes
- Inflammatory : Appendicitis, Diverticulitis, Ischemic colitis, Solitary rectal ulcer, Eosinophilic gastroenteritis, Graft-versus-host disease.
- Neoplastic : Lymphoma, Metastatic carcinoma, Carcinoma of the ileum, Familial polyposis.
- Drugs and chemicals : NSAIDs, Cathartic colon, Gold, Oral contraceptives, Cocaine, Chemotherapy.
References
- Harrison's Principles of Internal Medicine (21st edition), Loscalzo, Fauci, Kasper, Hauser, Longo, Jameson, The McGraw-Hill Companies.
- The image used in the cover is licensed under the Creative Commons Attribution-Share Alike 4.0 International license. (Author : WolfpackBME, Source : Wikimedia commons).
*This article is an excerpt from the above mentioned book and Medical Sutras does not make any ownership or affiliation claims.