Hyperventilation can be defined as ventilation in excess of that required to maintain normal arterial oxygen and carbon dioxide tension, produced by an increase in the frequency or depth of respiration or both.
Etiology
- Extreme anxiety (most common) : In dental practice, hyperventilation most often occurs in apprehensive patients, who hide their fears from doctors and attempt to "tough it out".
- Pain.
- Metabolic acidosis.
- Drug intoxication.
- Hypercapnia.
- Cirrhosis.
- Organic CNS disorders.
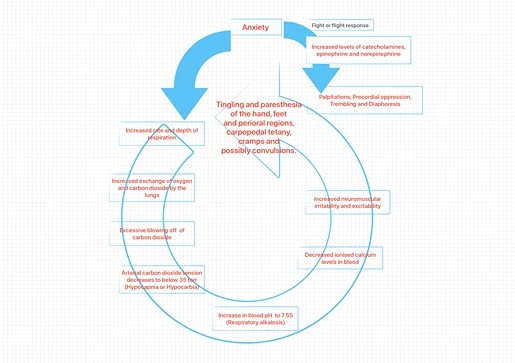
Pathogenesis

Clinical Manifestations
- Cardiovascular : Palpitations, Tachycardia, Precordial pain.
- Neurologic : Dizziness, Lightheadedness, Disturbance of conciousness, Disturbance of vision, Numbness and tingling of extremities, Tetany (rare).
- Respiratory : Shortness of breath, Chest pain, Dryness of mouth.
- Gastrointestinal : Globus hystericus, epigastric pain.
- Musculoskeletal : Muscle pain and cramps, Tremor, Stiffness and Carpopedal tetany.
- Psychological : Tension, Anxiety and Nightmares.
- Respiratory rate : Elevates to 25-30 breaths per minute (Normal 14-18 breaths per minute).
Management
In hyperventilation, the goal is to raise the carbon dioxide level in blood, which ends most of the symptoms.
-
Terminate the dental procedure and remove any foreign bodies from patient's mouth.
-
Position the patient in a semi-erect or upright position.
-
Any presumed cause (such as a syringe, dental handpiece or forceps), should be removed from the patient's line of vision.
-
Provide reassurance and calm the patient : Have the patient breathe slowly and regularly at a rate of about 4-6 breaths per minute, if possible.
-
If symptoms of alkalosis occurs, patient should be told to rebreathe exhaled air, which contains an increased concentration of CO2.
- Instruct the patient to cup his or her hands in front of the mouth and nose, and breathe in and out of it. (This also warms patient's cold hands and helps in alleviating one of the more frightening symptoms.)
- A full-face mask or paper bag can also be used.
- 100% oxygen is not indicated in hyperventilation : Administration of 100% oxygen or any enriched oxygen mixture, further decreases the arterial carbon dioxide level.
-
If hyperventilation continues, drug administration may be required to relieve patient's anxiety and slow the rate of breathing (Drug of choice : Benzodiazepines)
- IV : Titration at 1 ml per minute, until the patient's anxiety is reduced and the patient is able to control his/her breathing.
- IM : Midazolam (3-5mg) is preferred over diazepam (10mg), since, diazepam is not water soluble and burns when injected intramuscularly.
- Oral administration of diazepam may be considered, as the latent period for diazepam is actually longer after IM administration. (Oral dose of 10-15 mg diazepam usually terminates hyperventilation within 30 minutes.)
-
Monitor the vital signs.
-
Once hyperventilation stops, the patient should be rescheduled, with plans to use preoperative anxiolytics or intra-operative sedation (or both) in future visits.
References
- Medical Emergencies in the Dental Practice (7th edition), Stanley F. Malamed, Daniel L Orr II, Mosby Elsevier.
- Contemporary Oral and Maxillofacial Surgery (6th edition), James R Hupp, Edward Ellis III, Myron R Tucker, Mosby Elsevier.
*This article is an excerpt from the above mentioned books and Medical Sutras does not make any ownership or affiliation claims.