The common benign tumors of stomach includes gastric lymphoma, gastric polyps, gastric leiomyoma and adenocarcinoma of the stomach.
Etiology
-
H. pylori may be responsible for 60-70% cases.
-
Other factors associated with the risk of cancer :
- Diet rich in salted, smoked or pickled foods.
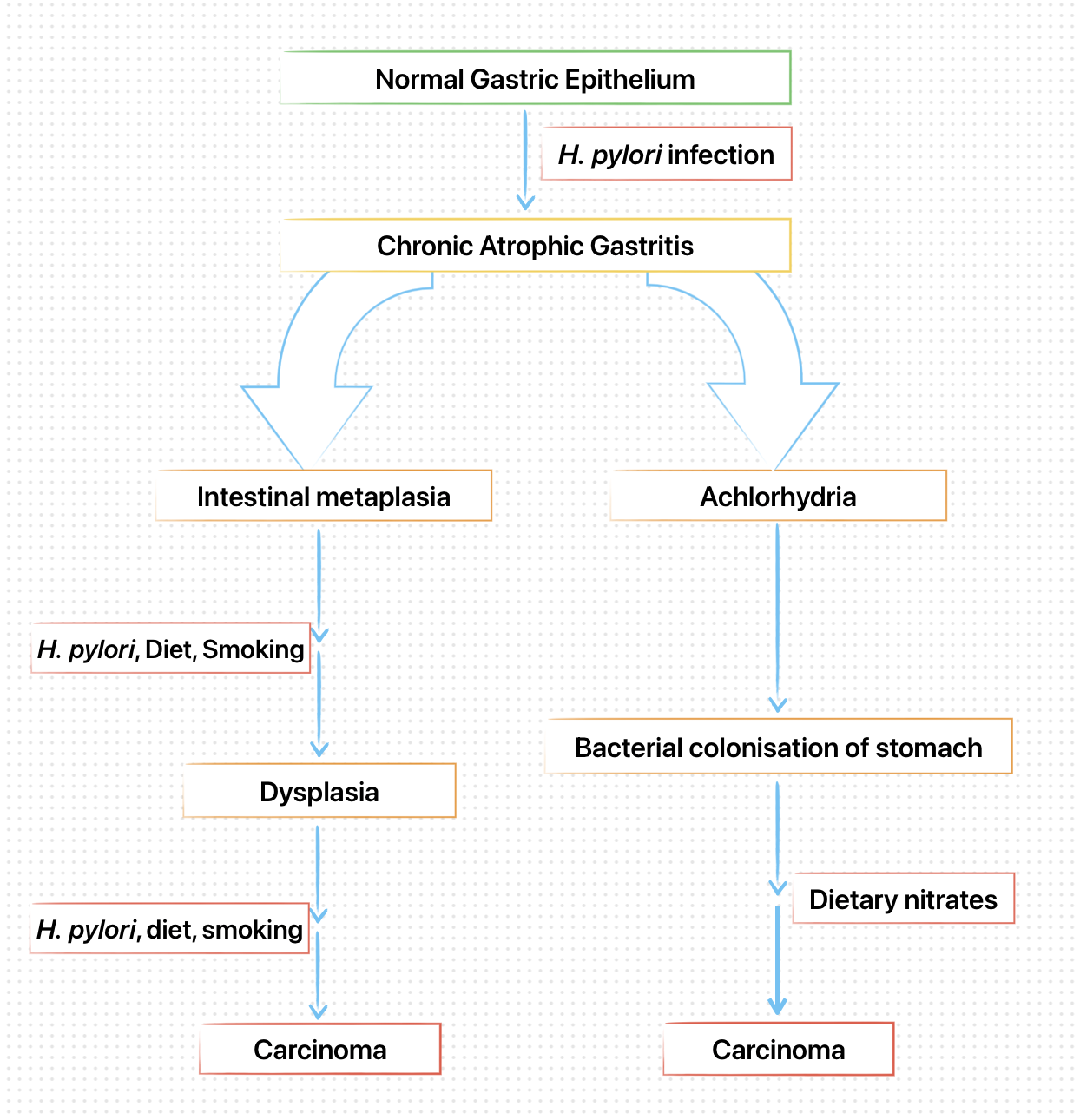
- Consumption of nitrites and nitrates : Carcinogenic N-nitroso compounds are formed from nitrates by the action of nitrite reducing bacteria which colonise the achlorhydric stomach.
- Diet lacking fresh fruits and vegetables as well as Vitamin C and A.
- Smoking and alcohol consumption.
- Autoimmune gastritis (pernicious anemia).
- Adenomatous gastric polyps.
- Previous partial gastrectomy.
- Menetrier's disease.
- Familial adenomatoids polyposis.
Pathology
- Virtually, all tumors are adenocarcinomas, that arise from mucus-secreting cells in the base of the gastric crypts.
- They mostly develops upon a background of chronic atrophic gastritis with intestinal metaplasia and dysplasia.
- The carcinoma can be either intestinal, arising from areas of intestinal metaplasia with histological features suggestive of intestinal epithelium, or diffuse, arising from normal gastric mucosa.
- Location : Antrum (50%), Gastric body (20-30%).
- Macroscopically, tumors can be classified as polypoid, ulcerating, fungating or diffuse.
Possible Mechanism of Carcinogenesis
Clinical Features
- Usually asymptomatic in early stages.
- Advanced cancers present with weight loss (in two-third cases), ulcer-like pain (in 50% cases), and anorexia and nausea (one-third cases).
- Dysphagia occurs in tumors of the gastric cardia which obstruct the gastroesophageal junction.
- Anemia (common, due to occult bleeding).
- Jaundice or ascites may signify metabolic spread.
- Occasionally, tumor spread occurs to the supraclavicular lymph nodes (Troisier's sign), umbilicus (Sister Joseph's nodule) or ovaries (Krukenberg tumor).
- Metastasis occurs most commonly in the liver, lungs, peritoneum and bone marrow.
Investigations
- Upper gastrointestinal endoscopy: Investigation of choice, should be performed promptly in any dyspeptic patient with 'alarm features'.
- Multiple biopsies, from the edge and base of gastric ulcer are required.
- Exfoliative brush cytology, also improves the diagnostic yield.
- Once diagnosis is made, further imaging is necessary for accurate staging and assessment of resectability.
Management
Surgical resection
- Offers the only hope of cure, that can be achieved in 90% of patients with early gastric cancer.
- Radical and total gastrectomy with lymphadenectomy (preserving the spleen, if possible) : Operation of choice for majority of patients who have locally advanced disease.
Neoadjuvant chemotherapy (based on 5-fluorouracil) may improve survival rates, although post-operative radiotherapy has no value.
Unresectable tumors
- The management of inoperable, locally advanced cancer is unsatisfactory.
- Moderate palliation of symptoms can be achieved in some patients with chemotherapy using FAM (5-fluorouracil, doxorubicin and mitomycin C) or ECF (epirubicin, cisplatin and 5-fluorouracil).
References
- Harrison's Principles of Internal Medicine (21st edition), Loscalzo, Fauci, Kasper, Hauser, Longo, Jameson, The McGraw-Hill Companies.
- The image used in the cover comes from Wellcome Images, a website operated by Wellcome Trust, a global charitable foundation based in the United Kingdom.
*This article is an excerpt from the above mentioned book and Medical Sutras does not make any ownership or affiliation claims.