Foreign body airway obstruction can be divided into two categories : Complete and Partial obstruction.
Partial obstruction can further be subdivided as :
- Partial obstruction with good air exchange.
- Partial obstruction with poor air exchange.
Complete airway obstruction
Complete airway obstruction presents the following clinical manifestations:
Phase 1 (Initial 3 minutes)
- The patient is conscious but in distress.
- Unable to make sounds or breath.
- Marked increase in sympathetic outflow, that leads to increase in BP, heart rate and respiratory rate.
- Exaggerated respiratory movements without air exchange.
- Decreased arterial oxygen tension, increase in arterial carbon dioxide tension and fall in pH.
- Retraction of supra-clavicular and intercostal muscles.
- Patient becomes cyanotic.
Phase 2 (3-4 minutes)
- Patient loses consciousness, with drop in BP and heart rate.
- Decreased respiratory efforts.
- Further deterioration in blood gases.
Phase 3 (After 4-5 minutes)
- Vital signs (BP and pulse) disappear.
- ECG degenerates from sinus to nodal bradycardia, then to idioventricular rhythms, and finally terminates in ventricular fibrillation or asystole.
- Full cardiorespiratory arrest.
Partial Airway Obstruction
Clinical manifestations in partial airway obstruction include:
With good air exchange
- Patient is able to breath and speak.
- Cough effectively.
- Wheezing between coughs.
With poor air exchange
- Weak, ineffectual cough or no cough.
- Crowing sound during inspiration.
- Markedly prolonged inspiratory phase.
- Inability to breathe or speak (Clutching the neck with the hands).
- Cyanosis, lethargy and disorientation.
Management in Children (older than 1 year) and Adults
- Terminate all dental procedures.
- Ask the patient to try to cough the object out.
- Identify complete airway obstruction (Universal sign of choking : Patient clutching at the neck).
- Ask "Are you choking ?" and "Can I help you ?".
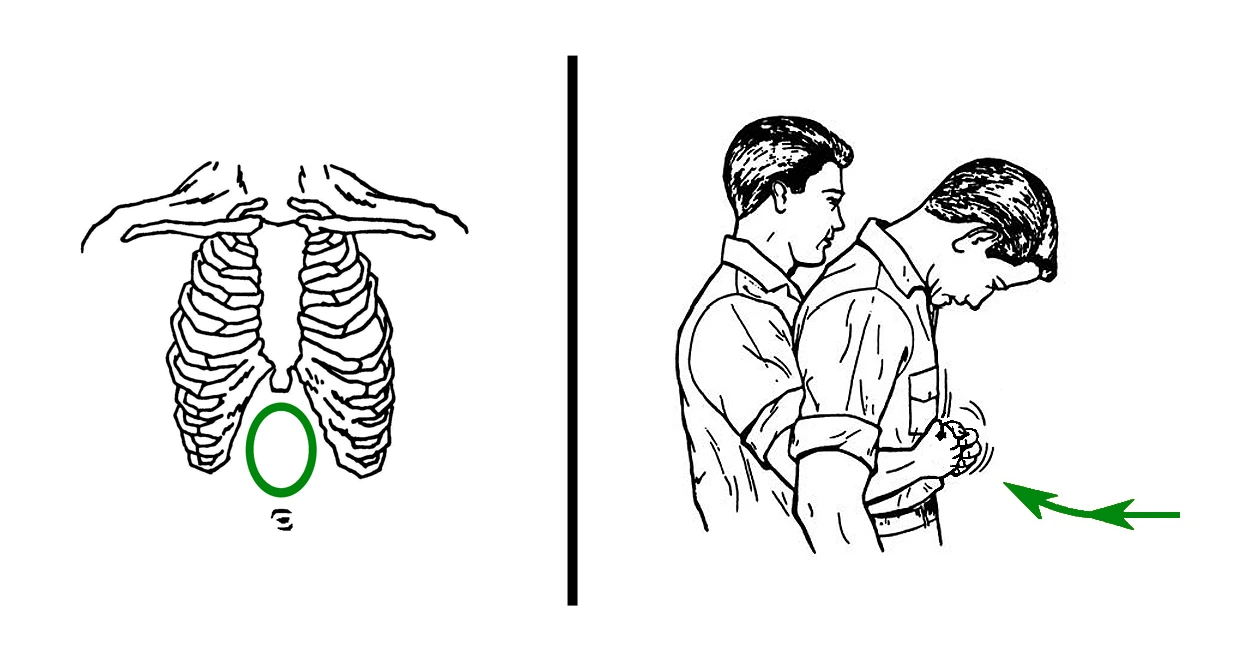
- Apply abdominal thrusts (Heimlich maneuvers) until the foreign body is expelled or the patient becomes unconscious.
If the foreign body is expelled
- Administer oxygen.
- Monitor vital signs.
- Shift to emergency care facility.
If patient becomes unconscious
- Place patient on the ground in supine position with head in neutral position
- Call for help and activate medical emergency services.
- Begin abdominal thrusts, followed by turning patient on side and using finger to sweep oral cavity for foreign body.
- Start BLS with 30 chest compressions.
- Every time you open the airway to ventilate, open the mouth wide and look for the foreign object.
- If visible, remove with fingers, Magill intubation forceps or other device.
- If not visible, continue chest compressions, looking into the mouth prior to ventilations for the object.
- Continue until effective or emergency medical service arrives to take over management.
If unable to ventilate (after 3 attempts)
- Laryngoscopy or cricothyrotomy is recommended (to be done by trained professionals).
Management in Infants (Under 1 year of age)
Conscious Infant : Combination of back slaps and chest thrusts are recommended.
- Kneel or sit with the infant placed on lap and remove clothing from infant's chest (if possible).
- Hold the infant with face down and head slightly lower than the chest, resting on the forearm.
- The infant's head and jaw should be supported by the arm and any compressing of the soft tissues of the infant's throat should be avoided.
- Deliver upto five back slaps forcefully between the infant's shoulder blades, using the heel of your hand. Each back slap should be forceful enough to dislodge the foreign body.
- Following five back slaps, place the free hand on the infant's back, supporting back of the infant's head with the palm.
- The infant should be protectively cradled between both the forearms with one palm supporting the back of the infant's head while the other palm supports the head and jaw.
- The infant should be turned as a unit into a head-facing-up position with your forearm resting on your thigh. The infant's head should be kept lower than the trunk.
- Deliver upto five quick downward chest thrusts in the middle of the chest over the lower half of the infant's sternum. This is the same hand placement as for infant chest compression during CPR.
- Chest thrust are delivered at a rate of 1 per second with each one strong enough to dislodge the foreign body.
- Repeat the sequence of five back slaps and five chest thrusts until the foreign body is removed or the infant loses consciousness.
Unconscious Infant : Back slaps are stopped and BLS commenced with chest compressions.
- Call for help and active emergency medical services immediately.
- Place the infant on a flat, firm surface.
- Begin chest compressions.
- At the completion of 30 compressions, inspect infant's mouth for the foreign body.
- If visible, remove the object using fingers or Magill intubation forceps.
- Continue CAB sequence for 2 minutes (5 cycles).
- Monitor vital signs and shift to a emergency care facility.
Points to Note
-
Most airway obstructions occur during inspiration, hence, the lungs are inflated and filled with oxygen that keeps the victim conscious for a longer time.
-
Blind finger sweeps should not be performed, as they may force the foreign body farther back into the airway.
-
Abdominal thrusts are not recommended in infants younger than 1 year of age, as they may cause injury or organ damage (eg. to the liver or spleen).
-
Indications for chest thrusts :
- Infants (Less than 1 year of age).
- Pregnant patient (Chest thrust is less likely to cause regurgitation).
- Obese patient (If the rescuer is unable to encircle the patient's abdomen).
-
Chest thrusts are contraindicated in older patients.
-
The rescuer should never place his or her hand over the xiphoid process or the lower margins of the rib cage.
-
After successful management and relieve of airway obstruction, the patient should be evaluated by medical staff for any secondary injury (such as abdominal bleeding), before discharging the patient.
References
- Medical Emergencies in the Dental Practice (7th Edition), Stanley F. Malamed, Daniel L Orr II, Mosby Elsevier. https://amzn.to/4bsbBkf
- Contemporary Oral and Maxillofacial Surgery (6th Edition), James R Hupp, Edward Ellis III, Myron R Tucker, Mosby Elsevier. https://amzn.to/3HJehMO
- The image used is in public domain (Source : Wikimedia Commons).
*This article is an excerpt from the above mentioned books and Medical Sutras does not make any ownership or affiliation claims.