The term dry socket describes the appearance of the extraction socket when the pain begins.
There is delayed healing, often associated with the loss, lysis or breakdown of a fully formed blood clot prior to its maturation.
Incidence
- Routine extraction: Rare (2% of extractions).
- Removal of impacted mandibular third molars and other lower molars: Frequent (20% of extractions in some studies).
- Incidence is higher in females.
Etiology
The cause is not fully clear, but, it appears to be due to high levels of fibrinolytic activity in and around the tooth extraction socket, which results in lysis of the blood clot and subsequent exposure of bone.
- The high fibrinolytic activity may result from subclinical infections, inflammation of the marrow space, or other factors.
- Contributing factors: Use of oral contraceptives, smoking, increasing age, presence of pericoronitis, surgical time, surgical trauma, and compromised medical status.
Clinical Features
- Most common complaints: Pain, Bad odor, and Foul taste.
- Pain does not respond well to oral analgesics and often keeps the patient up all night. Also, it presents without the usual signs and symptoms of infection such as fever, swelling, and erythema.
- Pain develops 3-4 days after removal of the tooth.
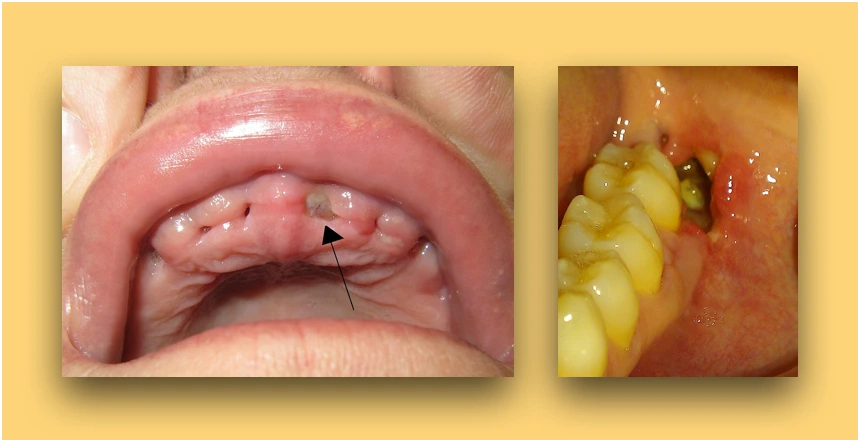
- On examination, the tooth socket appears to be empty, with a partially or completely lost blood clot. Food debris may or may not be present.
- Some bony surfaces of the socket are exposed. This exposed bone is sensitive and is the source of the pain.
- The site is tender on palpation, with the pain radiating to other areas of the head and neck including the ear, eye, or temporal and frontal regions.
- Intraoral radiograph should also be obtained to rule out the presence of a retained tooth structure or other surgical site complication, such as alveolar fracture.
Prevention
To prevent dry socket, the extraction should be performed with minimal trauma and bacterial contamination in the area of surgery.
- The extraction should be atraumatic with chlorhexidine gluconate 0.12% pre-surgical irrigation, clean incisions and soft tissue reflection.
- After the surgical procedure, the socket should be irrigated thoroughly with normal saline.
- Intra-alveolar antibiotics, specifically tetracycline, lincomycin, or clindamycin, placed alone or on a gelatin sponge, have shown to substantially decrease the incidence of dry socket.
- Postoperative antibiotics are not consistent in their ability to influence the development of dry socket and the evidence to support the use of systemic antibiotics is controversial.
Treatment
The condition is self-limiting, and the treatment is supportive. Treatment does not hasten healing and if the patient does not receive any treatment, there is no sequelae other than continued pain.
The primary goal is pain control and protecting the socket, until there is formation of adequate granulation tissue over the exposed socket walls.
- Firstly, the extraction socket needs to be gently irrigated with normal saline.
- Then, the socket is gently suctioned of all excess saline and a small strip of iodoform gauze soaked in or coated with medication is inserted into the socket with a small tag of gauze left trailing out of the socket.
- The patient usually experiences profound relief within 5 minutes, once the medicated gauze is inserted into the socket.
- The dressing should be changed every other day for the next 3-6 days, depending on the severity of pain. The socket is gently irrigated with saline at each dressing change.
- Once the patient's pain decreases, the dressing should not be replaced as it acts as a foreign body and further prolongs wound healing.
- Typically, there will be resolution of symptoms within 3-5 days, however, in certain cases it may take upto 14 days for complete resolution.
Points to Note
- The socket should not be curetted down to bare bone because this increases the amount of exposed bone and the pain. Usually, the entire blood clot is not lysed and the part that is intact should be retained.
- The medication mainly contains eugenol (obtunds the pain from the bone tissue), a topical anesthetic such as benzocaine, and a carrying vehicle such as Balsam of Peru.
- Eugenol is a member of the phenylpropanoid class of chemical compounds and causes inhibition of neural transmission and neurotoxicity.
- Iodoform is an organoiodine compound that has antibacterial property and is used as an antiseptic wound dressing.
- It is important to avoid the use of eugenol and other neurotoxic chemicals in the presence of an exposed inferior alveolar or lingual nerve.
- The use of systemic antibiotics is not recommended for the treatment of dry socket.
References
-
Contemporary Oral and Maxillofacial Surgery, 6th edition, James R Hupp, Edward Ellis III, Myron R Tucker, Elsevier.
-
Management of Complications in Oral and Maxillofacial Surgery, Michael Miloro, Antonia Kolokythas, Wiley-Blackwell.
-
Principles of Oral and Maxillofacial Surgery, 6th edition, U J Moore, Wiley-Blackwell.
-
Manual of Minor Oral Surgery for the General Dentist, 2nd edition, Pushkar Mehra, Richard D'Innocenzo, Wiley-Blackwell.
-
Oral and Maxillofacial Surgery, Lars Andersson, Karl-Erik Kahnberg, M Anthony Pogrel, Wiley-Blackwell.
-
Image Source: The files are licensed under the Creative Commons Attribution-Share Alike 3.0 Unported license.
- Dry socket 7 days after surgery (Author: Mel11691).
- Dry sockets post dental extraction in a person who smokes. (Author: James Heilman, MD).
*This article is an excerpt from the above mentioned books and Medical Sutras does not make any ownership or affiliation claims.