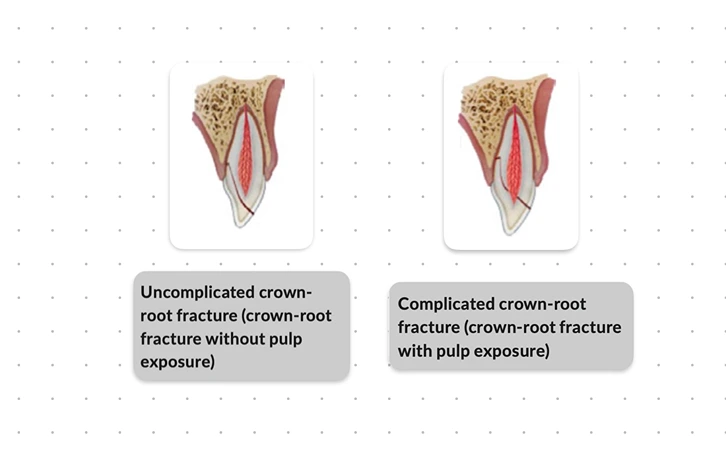
Crown root fracture is defined as a fracture involving enamel, dentin and cementum. It can be divided as complicated or uncomplicated depending on the involvement of pulp.
- Uncomplicated crown-root fracture: There is fracture involving enamel, dentin and cementum, without pulp exposure.
- Complicated crown-root fracture: There is fracture involving enamel, dentin and cementum, with pulp exposure.
Etiology
Crown-root fractures are usually caused by direct trauma in the anterior region and indirect trauma in the posterior region. The common etiologic factors include:
- Injuries caused by falls, automobile accidents and foreign body striking the teeth.
- Iatrogenic factors such as lateral pressure during root canal obturation, cementation of posts, corrosion of posts or improperly designed restorations.
Clinical Findings
- Positive pulp sensitivity tests.
- Presence of tenderness on percussion.
- Coronal (mesial or distal) fragment is usually present and mobile.
Radiographic Findings
-
Apical extension of the fracture is usually not visible.
-
Recommended radiographs:
- One parallel IOPA radiograph.
- Two additional radiographs of the tooth, with different angulations (vertical and/or horizontal).
- Radiographs of the lip and/or cheek : If the fragment is missing and there are soft tissue injuries.
- CBCT can be considered for better visualisation and treatment plan.
Immediate Management
Temporary stabilisation of the loose fragment to the adjacent tooth/teeth or to the non-mobile segment.
Uncomplicated crown-root fracture
- Remove the coronal or mobile (loose) fragments and cover the exposed dentin with GIC or a bonding agent and composite resin.
Complicated crown-root fracture
- Immature tooth: Partial pulpotomy is recommended, so as to preserve the pulp. Non-setting Ca(OH)2 or non-staining calcium silicate cements are suitable for placement in the pulp wound.
- Mature tooth: Pulpectomy is usually indicated.
Definitive Management
In the permanent dentition, the definitive treatment is dependent on the site and type of fracture; patient's age and anticipated cooperation; and the cost and complexity of treatment. Treatment options include:
- Removal of coronal fragment and supragingival restoration.
- Surgical exposure of the fracture surface.
- Orthodontic extrusion of apical fragment.
- Surgical extrusion of apical fragment.
- Vital root submergence.
- Extraction of the tooth.
Removal of coronal fragment and supragingival restoration
- The tooth is restored temporarily to allow gingival healing (presumably with formation of long junctional epithelium), after which permanent restoration is done.
- Indication: Superficial fractures, not involving the pulp.
- Procedure: Loose fragments are removed, rough edges smoothened and the crown is temporarily restored supragingivally. After 2-3 weeks, once the gingival tissue heals, crown is restored with a dentin and enamel-bonded composite.
Surgical exposure of the fracture surface
- The subgingival fracture is converted to a supra-gingival fracture, with the help of gingivectomy and osteotomy.
- Indication: Where the coronal fragment comprises one third or less of the clinical root.
- Procedure: The coronal fragment is removed and the surface is carefully examined for any secondary fracture. The fracture surface is exposed using gingivectomy and osteotomy and the tooth is restored with a post-retained porcelain jacket crown.
- Poor long-term prognosis: Due to development of a pathologic pocket palatally and inflammation of surrounding gingiva, as regrowth of the gingiva often takes place. After some years, this can result in labial migration of the restored teeth (about 0.8 mm over 5 years).
Orthodontic extrusion of apical fragment
-
The fracture is moved to a supra-gingival position orthodontically.
-
Indication: Recommended for uncomplicated crown-root fractures, wherein
- coronal fragment comprises one third or less of the clinical root,
- vitality of the pulp is to be preserved,
- it is desirable to reconstruct osseous and/or gingival defects (slow orthodontic extrusion can act as guide for downgrowth of these tissues).
-
Procedure: Loose fragments are removed and the tooth is endodontically treated. The fracture surface is exposed via orthodontic extrusion of the root. Once the root is extruded, gingivectomy or osteotomy is done to restore symmetry of gingival contour. The tooth is restored temporarily and splinted to adjacent teeth for retention upto 6 months. After retention period, the tooth is restored permanently.
-
Endodontic considerations
- Mature tooth: Pulpectomy and RCT.
- Immature tooth: Pulp capping or pulpotomy.
Surgical extrusion of apical fragment
- The fracture is surgically moved to a supra-gingival position.
- Indication: Should be used only in mature tooth with complete root formation, where the apical fragment is long enough to accommodate a post-retained crown (the coronal fragment comprises less than half root length.).
- Procedure: The PDL fibres are incised, followed by luxation and extraction of tooth with an elevator. Root surface is inspected for incomplete root fracture and in the absence of any, the root is repositioned at a level 1 mm coronal to the alveolar crest. Tooth is stabilised using inter-proximal sutures. After 2-3 weeks, the transplant is usually firm and a temporary restoration is fabricated. After 6 months, a permanent root filling and definitive crown restoration is completed.
- Endodontic treatment can be done initially before surgical extrusion or postponed for 2-3 weeks, once the tooth becomes firm. If the root filling is done prior to transplantation, tooth can be restored after 2 months.
Vital root submergence
- Root portion of the fractured tooth is kept in place to maintain width and height of the alveolar ridge.
- Indication: Young individuals, where the fractured tooth cannot be restored.
- Procedure: A surgical flap is raised, the supra-alveolar fragments of the tooth are removed and the flap is closed over the exposed root including the pulp.
Extraction of the tooth
-
Indication:
- When no other treatment is indicated.
- The coronal fragment comprises more than one third of the clinical root.
- Vertical crown-root fracture.
-
Disadvantage: There is rapid resorption of the supporting bone.
-
In patient who have completed growth, implant treatment is a good alternative.
-
In growing patients, orthodontic space closure or autotransplantation are better alternatives.
Prognosis
Clinical and radiographic evaluations (follow up) are necessary at 1 week, 6-8 weeks, 3 months, 6 months, 1 year and then yearly for at least 5 years.
Favourable Outcomes
- Asymptomatic.
- Positive response to pulp sensitivity testing (in uncomplicated fractures).
- Continued root development in immature teeth.
Unfavourable Outcomes
- Persistence of symptoms.
- Tooth discolouration (in uncomplicated fractures).
- Pulp necrosis and infection.
- Apical periodontitis.
- Lack of further root development in immature teeth.
- Loss or breakdown of restoration.
- Marginal bone loss and periodontal inflammation.
Points to Note
- Fracture healing cannot be expected in crown-root fractures, since, the oral cavity and the PDL or pulp are connected by the fracture line and this allows bacterial invasion and subsequent inflammation.
- If the goal of extrusion is a crown-root ratio of approximately 1:1, central incisor can be extruded 2-4 mm, while lateral incisor can be extruded 4-6mm.
- Autotransplantation : Transplantation of a donor tooth to the site of traumatic tooth loss.
References
- Textbook and Color Atlas of Traumatic Injuries to the Teeth, Jens O. Andreasen, Frances M. Andreasen, Lars Andersson.
- Bourguignon C, Cohenca N, Lauridsen E, et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations. Dent Traumatol. 2020;36:314–330. https://doi.org/10.1111/edt.12578.
*This article is an excerpt from the above mentioned sources and Medical Sutras does not make any ownership or affiliation claims.