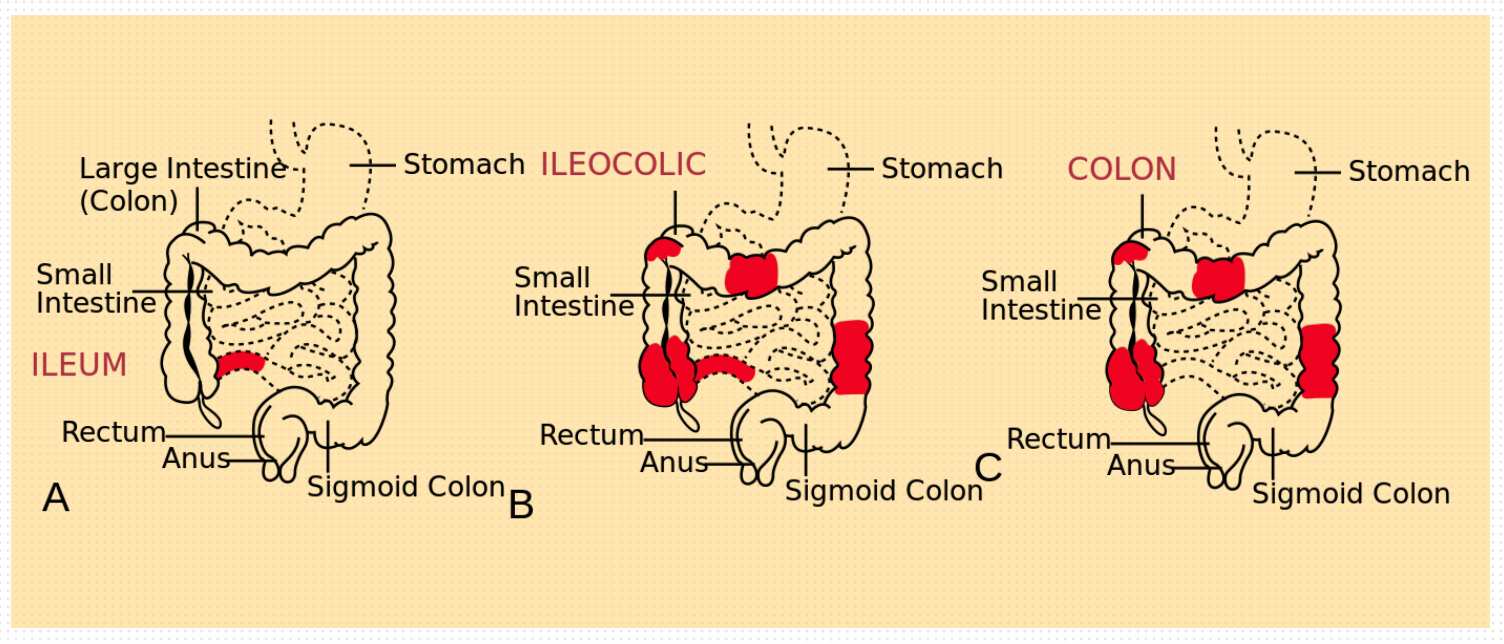
Crohn's disease (CD) can affect any part of the gastrointestinal tract from the mouth to the anus, with the rectum often not involved (in contrast to ulcerative colitis). It is transmural in nature i.e., all layers of the bowel may be inflamed.
Macroscopic Features
CD presents as segmental (skip) lesions, with skip areas (normal gut) in the midst of diseased intestine, and one-third of patients present with peri-rectal fistulas, fissures, abscesses and anal stenosis (particularly those with colonic involvement).
Endoscopic findings include,
-
Cobblestone appearance : Stellate ulcerations fuse longitudinally and transversely to demarcate islands of mucosa that are frequently normal histologically. It is characteristic of CD, both endoscopically and by barium radiography.
-
Mild disease : Aphthous or small superficial ulcerations.
-
Active CD
- Focal inflammation and formation of fistula tracts, which resolve by fibrosis and stricturing of the bowel.
- The bowel wall thickens and becomes narrowed and fibrotic, leading to chronic, recurrent bowel obstructions.
- Creeping fat : Refers to the projections of the thickened mesentery that encase the bowel.
- Adhesions and fistula formation (promoted by the serosal and mesenteric inflammation).
Microscopic Features
- Earliest lesions : Aphthoid ulcerations and focal crypt abscesses with loose aggregations of macrophages, which from non-caseating granulomas in all layers of the bowel wall (from mucosa to serosa).
- Granulomas can be seen in lymph nodes, mesentery, peritoneum, liver and pancreas.
- Submucosal or subserosal lymphoid aggregates, particularly away from areas of ulceration.
- Gross and microscopic slip areas.
- Transmural inflammation, accompanied by fissures that penetrate deeply into the bowel wall and sometimes form fistulous tracts or local abscesses.
Signs and Symptoms
Although CD usually presents as acute or chronic bowel inflammation, the inflammation process evolves toward one of two patterns of disease : a fibrostenotic obstructing pattern or a penetrating fistulous pattern, each with different treatments and prognoses.
Ileocolitis
The usual presentation is a chronic history of recurrent episodes of right lower quadrant pain and diarrhoea. Sometimes, the initial penetration mimics acute appendicitis with pronounced right lower quadrant pain, a palpable mass, fever, and leukocytosis.
-
Pain : Usually colicky, it precedes and is relieved by defecation.
-
Low-grade fever.
-
Weight loss : Typically 10-20% of body weight, develops as a consequence of diarrhoea, anorexia and fear of eating.
-
Palpation : An inflammatory mass may be palpated in the right lower quadrant of the abdomen. The mass is composed of inflamed bowel, adherent and indurated mesentery and enlarged lymph nodes. Extension of the mass can cause obstruction of the right ureter or bladder inflammation, manifested by dysuria and fever.
-
String sign : The lumen resembles a frayed cotton string in radiographs. It results from a severely narrowed loop of bowel, caused by incomplete filling of the lumen due to edema, irritability, and spasms associated with inflammation and ulcerations.
-
Bowel obstruction : May take several forms.
- Early stage : Intermittent obstructive manifestations and increasing symptoms of post-prandial pain, due to bowel wall edema and spasm.
- Late stage : Persistent inflammation gradually progresses to fibrostenotic narrowing and stricture. Diarrhoea will decrease and be replaced by chronic bowel obstruction.
-
Severe infection may lead to localised wall thinning, with microperforation and fistula formation to the adjacent bowel, the skin, the urinary bladder, or to an abscess cavity in the mesentery.
- Enterovisceral fistula : Present as dysuria or recurrent bladder infections or less commonly, as pneumaturia or fecaluria.
- Enterocutaneous fistula : Follow tissue planes of least resistance, usually draining through abdominal surgical scars.
- Enterovaginal fistula : Rare and present as dyspareunia or as a feculent or foul-smelling, often painful vaginal discharge (unlikely to develop without a prior hysterectomy).
Jejunoileitis
Associated with a loss of digestive and absorptive surface, resulting in malabsorption and steatorrhea.
-
Nutritional deficiencies can also result from poor intake and enteric losses of protein and other nutrients.
-
Intestinal malabsorption can cause hypoalbuminemia, hypocalcemia, hypomagnesemia, coagulopathy and hyperoxaluria with nephrolithiasis in patients with an intact colon.
-
Vertebral fractures : Caused by a combination of Vitamin D deficiency, hypocalcemia and prolonged glucocorticoid use.
-
Pellagra (niacin deficiency) : Can occur in extensive small-bowel disease.
-
Megaloblastic anemia and neurologic symptoms : Due to malabsorption of vitamin B12.
-
Diarrhoea : Characteristic of active disease. Its causes include,
- Bacterial overgrowth in obstructive stasis or fistulisation.
- Bile acid malabsorption due to a diseased or resected terminal ileum.
- Intestinal inflammation with decreased water absorption and increased secretion of electrolytes.
- Enteroenteric fistula.
Colitis and Perianal Disease
Patients with colitis present with low-grade fevers, malaise, diarrhoea, crampy abdominal pain and sometimes hematochezia.
- Gross bleeding : Occurs in about half of the patients with exclusively colonic disease.
- Pain is caused by passage of fecal material through narrowed and inflamed segments of large bowel. Decreased rectal compliance is another cause for diarrhoea in Crohn's colitis patients.
- Stricturing can occur in the colon (4-16%) and produce symptoms of bowel obstruction.
- Also, colonic disease may fistulize into the stomach or duodenum, causing feculent vomiting, or to the proximal or mild small bowel, causing malabsorption by short circuiting the absorptive surface and bacterial overgrowth. Rectovaginal fistula is seen in 10% of women.
Gastroduodenal disease
Signs and symptoms of upper gastrointestinal tract disease include nausea, vomiting and epigastric pain.
- Patients usually have H. pylori negative gastritis.
- Fistulas involving the stomach or duodenum arise from the small or large bowel and do not necessarily signify the presence of upper g.i. tract involvement.
- Patients with advanced gastroduodenal CD may develop a chronic gastric outlet obstruction.
Investigations
Investigations include laboratory testing, endoscopy and radiography.
Laboratory findings
- Elevated ESR and C-reactive protein (CRP).
- In more severe disease, hypoalbuminemia, anemia and leukocytosis.
- Fecal calprotectin and lactoferrin levels : Used to distinguish IBD from IBS, to assess whether CD is active and to detect postoperative recurrence of CD.
Endoscopic findings
- Rectal sparing, aphthous ulcerations, fistulas and skip lesions.
- Wireless capsule endoscopy (WCE) allows direct visualisation of the entire small-bowel mucosa.
- Endoscopic appearance correlated poorly with clinical remission, thus, repeated endoscopy is not used to monitor the inflammation.
Radiographic findings
- Early radiographic findings in the small bowel include thickened folds and aphthous ulcerations. Cobblestoning from longitudinal and transverse ulcerations most frequently involves the small bowel.
- More advanced disease : Strictures, fistulas, inflammatory masses, and abscesses may be detected.
- The transmural inflammation of CD leads to decreased luminal diameter and limited distensibility. As ulcers progress deeper, they can lead to fistula formation.
- String sign : Represents long areas of circumferential inflammation and fibrosis, resulting in long segments of luminal narrowing.
- The segmental nature of CD result in wide gaps of normal or dilated bowel between involved segments.
- MRI : Offers superior soft tissue contrast and has the added advantage of avoiding radiation exposure changes (particularly appealing in younger patients and when serial images needs to be obtained for monitoring response to therapy).
- Small-bowel ultrasound (SBUS) : Underutilised but as sensitive as MR enterography and CT enterography for detecting small-bowel CD. Use of oral contrast medium can increase the sensitivity and specificity to 100%. SBUS is best suited for distal small-bowel assessment.
Complications
- Serosal adhesions provide direct pathways for fistula formation and reduce the incidence of free perforation (1-2%).
- Intra-abdominal and pelvic abscess (10-30%) : CT-guided percutaneous drainage is standard therapy, however, most patients need resection of the offending bowel segment.
- Intestinal obstruction (40%).
- Massive haemorrhage.
- Malabsorption and severe perianal disease.
References
- Harrison's Principles of Internal Medicine (21st edition), Loscalzo, Fauci, Kasper, Hauser, Longo, Jameson, The McGraw-Hill Companies.
- The image used in the cover is licensed under the Creative Commons Attribution-Share Alike 3.0 Unported license. Author : Samir, vectorized by Fvasconcellos, Source : w:Image:Patterns of CD.jpg (Wikimedia commons).
*This article is an excerpt from the above mentioned book and Medical Sutras does not make any ownership or affiliation claims.