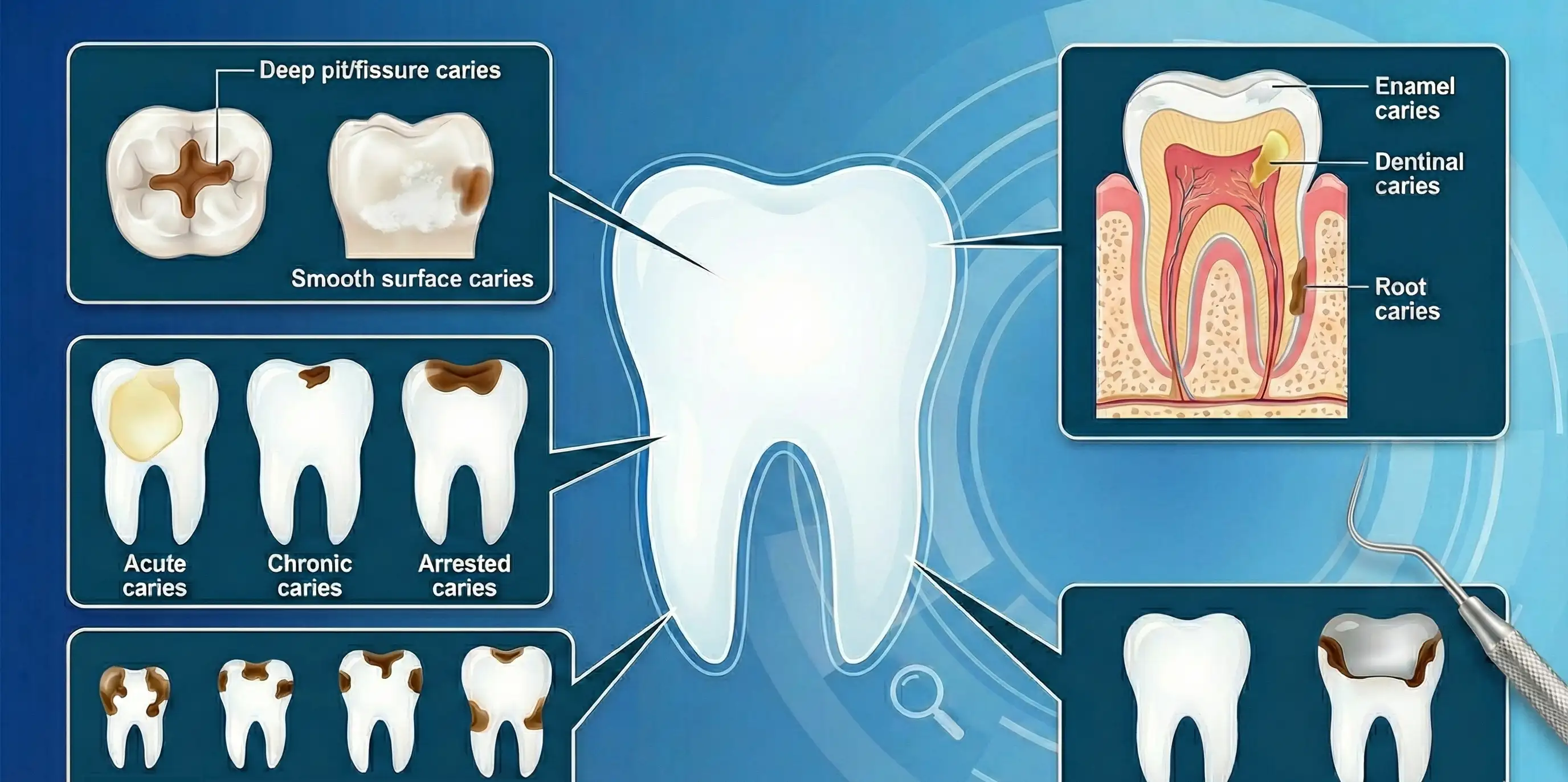
There are several classification of dental caries based on different criteria. These include:
- Location/Anatomical site: Pit or fissure and Smooth surface caries.
- Extension: Enamel, Dentinal and Root caries.
- Severity: Acute, Chronic and Arrested caries.
- Chronology: Early childhood, Teenage, Adolescent, and Adult caries.
- Origin: Primary and Secondary caries.
Based on Location or Anatomical Site
Pit or Fissure Caries
-
It involves carious lesion present on the pits and fissures of the tooth. Common sites include the occlusal surface of molars and premolars, buccal and lingual surface of molars, and the lingual surface of maxillary incisors.
-
The pits and fissures favour retention of food debris and microorganisms, and form a niche for plaque accumulation. Also, these areas cannot be cleaned while brushing as the bristles cannot reach. Thus, they are highly susceptible to caries.
-
The affected pits and fissures may appear brown or black, and the bordering enamel bluish white as it becomes undermined.
-
On probing with explorer, the caries will feel slightly soft and it will catch the explorer point.
-
The caries often starts at both sides the fissure wall and extends perpendicularly towards the dentinoenamel junction. The caries follows the direction of enamel rods that flare laterally from the pit to the DEJ. This results in characteristic triangular shaped lesion with the apex at the pit and base directed towards dentin.
-
Pits and fissures can be of two types:
- Shallow, wide V or U shaped fissures: Self cleansing.
- Deep, narrow I shaped fissures: Constricted with narrow slit like opening. These may have lateral branches and appear as K, Y or inverted Y shaped.
Smooth Surface Caries
- It affects the smooth surface of the tooth such as the proximal surface or the gingival third of buccal and lingual surfaces.
- Proximal caries usually begin just below the contact areas, while cervical caries presents as cresent-shaped cavity extending from the area opposite the gingival crest to the convexity on the tooth surface.
- They start with a white chalky spot or faint white opacity that becomes slightly roughened as there is superficial decalcification of enamel. Then, as the caries penetrates the enamel, the surrounding enamel becomes bluish white in appearance.
Based on Extension
Enamel Caries
- It refers to the caries limited to the enamel.
- It presents a small, opaque white region called 'white spot'. The enamel overlying this white spot is hard and shiny, similar to sound enamel. However, there is mineral loss and demineralisation 10-15mm beneath the outer surface (subsurface enamel caries), which leads to the formation of the white spot.
- It may also appear brownish due to exogenous stain, and referred as 'brown spot lesion'.
Dentinal Caries
- These extend into the dentin.
Root caries
- It refers to the caries involving the roots of teeth.
Based on Severity
Acute Dental Caries
- It runs a rapid clinical course and results in early pulp involvement.
- There is no secondary dentin formation as the process is rapid.
- The carious dentin is usually stained light yellow.
- E.g., nursing bottle caries and rampant caries.
Chronic Dental Caries
- It progresses slowly and tends to involve the pulp at much later stage.
- The slow progress of caries allows sufficient time for deposition of secondary dentin, resulting in a shallow cavity with minimum softening of dentin.
- The caries dentin often stains deep brown.
Arrested Caries
- It is a static or stationary form of caries that does not show any tendency towards further progression.
- It is usually seen in occlusal surface caries and is characterised by a large open cavity. This large open cavity does not allow any food retention and the superficial softened and decalcified dentin is gradually burnished until it becomes hard. The dentin appears brown and polished, and is referred as 'eburnated dentin'.
Based on Chronology
Early Childhood Caries
- Commonly known as Nursing Bottle Caries or Baby Bottle Tooth Decay.
- It occurs in infants and very young children, often due to prolonged exposure to sugary liquids (milk, formula, fruit juice) from a bottle or sippy cup, especially during sleep.
- It typically affects the maxillary (upper) incisors first, while the mandibular (lower) incisors are often spared because they are protected by the tongue and bathed in saliva.
Adolescent Caries
- This is a rapid form of decay seen during the teen years.
- It is often linked to the frequent consumption of "sticky" carbohydrates and sugary soft drinks, combined with hormonal changes and sometimes a decrease in oral hygiene diligence.
- It frequently presents as small surface openings that hide extensive destruction of the underlying dentin.
Adult Caries
- Usually manifests as a slower, more chronic progression.
- In older adults, this often transitions into Root Caries as gingival recession exposes the cementum, which is less mineralized than enamel and more susceptible to decay.
Based on Origin
This distinguishes whether the decay is occurring for the first time or returning to a previously treated area.
Primary (Virgin) Caries
- A carious lesion that occurs on a tooth surface that has never been restored or affected by decay before.
- It represents the initial attack of the disease on the natural tooth structure.
Secondary/Recurrent Caries
- This occurs at the margins or borders of an existing restoration (filling, crown, etc.).
- It is typically caused by "microleakage", the seepage of bacteria and food debris into the tiny gap between the tooth and the filling material.
- This can happen due to poor initial adaptation of the material, chipping of the restoration, or the natural breakdown of dental cements over time.
Radiation Caries
- It is a rapid and highly destructive form of decay observed in patients who have undergone radiotherapy for head and neck cancers.
- It is not caused directly by the radiation hitting the teeth, but rather by the permanent damage done to the salivary glands (Xerostomia or dry mouth). Without the buffering and cleaning action of saliva, the teeth demineralize at an accelerated rate.
- It typically starts at the cervical (neck) region of the teeth and can progress so rapidly that the entire crown of the tooth may eventually break off, leaving only the roots.
References
- Arathi Rao, Principles and Practice of Pedodontics, 3rd Edition, Jaypee Brothers Medical Publishers (P) Ltd.
- Image Source: Google Gemini.
*This article is an excerpt from the above mentioned sources and Medical Sutras does not make any ownership or affiliation claims.