Avulsion or Exarticulation is the complete displacement of the tooth out of its socket. It represents a true emergency situation in dentistry and the prognosis is very much dependent on the actions taken at the place of accident.
First Aid (Management at the place of avulsion)
Immediate replantation of the avulsed tooth is the best treatment at the place of accident. However, primary teeth should not be replanted.
- Keep the patient calm.
- Find the tooth (Pick it by the crown, avoid touching the root).
- If the tooth is dirty, it should be rinsed gently in milk, saline or patient's saliva and replanted it to its original position in the jaw.
- Once the tooth is replanted, the patient should be advised to bite on a gauze, handkerchief or napkin to hold it in place.
- If it is not possible or feasible to replant the tooth at the accident site (eg, an unconscious patient), the tooth should be placed in a storage or transport medium, as early as possible (to prevent dehydration of the root surface).
- The patient should visit the nearest dental facility for further management.
Treatment Guidelines
The choice of treatment is related to:
Maturity of Root
- Open or closed apex.
Condition of PDL cells: Dependent on the extraoral dry time and the storage medium (critical for survival of the PDL cells).
- PDL cells are most likely viable: Tooth is replanted immediately or within 15 minutes at the site of accident.
- PDL cells may be viable but compromised: Tooth has been kept in a storage medium (eg. milk, HBSS, saliva or saline) or total extraoral dry time is less than 60 minutes.
- PDL cells are likely to be non-viable: Extra-oral dry time more than 60 minutes (regardless of the storage medium).
Avulsed Permanent Tooth replanted immediately or within 15 minutes
-
The injured area should be cleaned with water, saline or chlorhexidine.
-
The correct position of the replanted tooth should be verified both clinically and radiographically. Any malpositioning should be corrected using slight digital pressure.
-
Administer local anesthesia, if necessary, and preferably with no vasoconstrictor.
-
If the tooth or teeth were replanted in the wrong socket or rotated, it should be repositioned into the proper location within 48 hours after trauma.
-
The tooth should be stabilised for 2 weeks using a passive flexible splint (eg, 0.016 inch or 0.4 sq. mm wire or Nylon fishing line, 0.13-0.25 mm) bonded to the tooth and adjacent teeth. A more rigid splint (for about 4 weeks) is indicated in case of associated alveolar or jawbone fracture.
-
Any gingival lacerations present should be sutured.
-
Endodontic Consideration:
- Closed apex: Root canal treatment within 2 weeks after replantation.
- Open apex: Pulp revascularization.
-
Status of tetanus immunization and boosters should be checked.
-
Prescribe systemic antibiotics and give post-operative instructions.
-
Follow up at regular intervals.
Avulsed Permanent Tooth with extraoral dry time less than 60 minutes
(Whether kept in a physiologic storage medium or stored in non-physiologic conditions.)
-
The avulsed tooth should be checked for any visible contamination and should be cleaned with a stream of sterile saline or by gently agitating in the storage medium.
-
The tooth can be left in the storage medium while taking patient history, clinical examination, radiography and preparing the patient for replantation.
-
Administer local anesthesia, if necessary, and preferably with no vasoconstrictor.
-
The alveolar socket should be irrigated with sterile saline and examined properly. If there is any fracture of the socket wall, it should be repositioned into its original position with a suitable instrument.
-
Any coagulum formed should also be removed from the socket to allow better repositioning of the tooth.
-
The avulsed tooth should be replanted slowly with slight digital pressure and the correct position be verified both clinically and radiographically. Excessive force should not be used.
-
The tooth should be stabilised for 2 weeks using a passive flexible splint (eg, 0.016 inch or 0.4 sq. mm wire or Nylon fishing line, 0.13-0.25 mm) bonded to the tooth and adjacent teeth. A more rigid splint (for about 4 weeks) is indicated in case of associated alveolar or jawbone fracture.
-
Any gingival lacerations present should be sutured.
-
Endodontic Consideration:
- Closed apex: Root canal treatment within 2 weeks after replantation.
- Open apex: Pulp revascularization.
-
Status of tetanus immunization and boosters should be checked.
-
Prescribe systemic antibiotics and give post-operative instructions.
-
Follow up at regular intervals.
Avulsed Permanent Tooth with extraoral dry time more than 60 minutes
Delayed replantation has a poor long-term prognosis, since the PDL becomes necrotic and is not expected to regenerate.
- The goal of replantation in these cases is to restore, at least temporarily, esthetics and function while maintaining alveolar bone contour, height and width. This helps to keep the future treatment options open.
- The tooth can always be extracted, if needed, and at appropriate point following prompt inter-disciplinary assessment.
- The expected outcome of delayed replantation is ankylosis-related (replacement) root resorption.
- The steps involved are similar to those mentioned above for extra-oral dry time less than 60 minutes.
Storage Media
The recommended storage mediums in descending order of preference are:
- Milk.
- Hank's Balanced Salt Solution (HBSS).
- Saliva.
- Saline.
- Water (Poor medium, but better than leaving the tooth to air-dry).
Isotonic saline or pasteurised whole bovine milk are the most favorable storage medium. If neither of them is not readily available, human saliva is preferable.
Antibiotic Considerations
Systemic Antibiotics
-
Amoxicillin: First choice due to their effectiveness on oral flora and very few side effects.
-
Tetracyclines:
- Doxycycline is appropriate because of its antimicrobial, anti-inflammatory and anti-resorptive effects.
- Tetracycline or doxycycline are generally not recommended for patients under 12 years of age.
Topical Antibiotics
- The effect of topical antibiotics placed on the root surface prior to replantation with respect to pulp revascularization remains controversial.
- While animal studies have shown great potential, human studies have failed to demonstrate improved pulp revascularization when teeth are soaked in topical antibiotics.
Endodontic Considerations
Closed Apex
- RCT should be initiated within 2 weeks post replantation.
- Calcium hydroxide is recommended as intracanal medicament for up to 1 month followed by root canal filling.
- If a corticosteroid or corticosteroid/ antibiotic mixture is chosen to be used as an anti-inflammatory and anti-resorptive intracanal medicament, it should be placed immediately or shortly after replantation and left in situ for at least 6 weeks.
Open Apex
- In immature teeth with open apices, pulp revascularization is recommended, since, spontaneous healing can occur in the form of new connective tissue with vascular supply. This allows continued root development and maturation.
- In cases where spontaneous revascularization does not occur and pulp necrosis and infection of the root canal system are identified, it is recommended to initiate apexification, pulp space revascularization/ revitalisation or RCT.
- The risk of external infection-related (inflammatory) root resorption should be weighed against the chances of revascularization since resorption is very rapid in children.
Post-operative Instructions
- Avoid participation in contact sports.
- Maintain a soft diet for up to 2 weeks, according to the tolerance of the patient.
- Brush the teeth with a soft toothbrush after each meal.
- Use chlorhexidine (0.12%) mouth rinse twice a day for two weeks.
- The patient or parents should be fully informed about the prognosis and the potential cost and time required for different treatment options.
Prognosis
Replanted teeth should be monitored clinically and radiographically at 2 weeks (when the splint is removed), 4 weeks, 3 months, 6 months, 1 year and yearly thereafter for at least five years.
Favorable Outcomes
- Asymptomatic, functional, normal mobility, no sensitivity to percussion and normal percussion sound.
- No radiolucencies and no radiographic evidence of root resorption.
- Open Apex: Radiographic evidence of continued root formation and tooth eruption. Pulp canal obliteration is expected and can be seen radiographically sometime during the first year after trauma.
Unfavorable Outcomes
- Presence of swelling or sinus tract.
- Tooth with excessive mobility or no mobility (ankylosis) with high-pitched (metallic) percussion sound.
- Presence of radiolucencies.
- Infection-related (inflammatory) resorption: Root and/or bone resorption anywhere around the circumference of the root.
- Ankylosis-related (replacement) resorption: Absence of PDL space, replacement of root structure by bone, together with a metallic sound to percussion.
- When ankylosis occurs in growing patient, infra-position of the tooth is highly likely to create disturbances in alveolar and facial growth over the short, medium and long term.
- Open Apex: Absence of continued root formation.
Points to Note
-
Most commonly avulsed tooth: Maxillary Central Incisor.
-
Most often avulsion involves a single tooth.
-
Avulsion injuries are three times more frequent in boys than girls.
-
Most common age group: 7-9 years (When permanent incisors are erupting : Andreasen suggests that the loosely structured PDL surrounding the erupting teeth favors complete avulsion).
-
A primary tooth should not be replanted because there are chances of subsequent damage to the permanent tooth germ and pulp necrosis.
-
Situations where replantation is not indicated
- Severe caries or periodontal disease.
- Uncooperative patient.
- Severe cognitive impairment requiring sedation.
- Severe medical conditions such as immunosuppression.
- Severe cardiac conditions.
-
Nylon fishing line is not recommended for children when there are only a few permanent teeth for stabilisation of the traumatised tooth. This stage of development may result in loosening or loss of the splint.
-
In immature tooth with open apex, obliteration of pulp canal is considered to be the mechanism by which the pulp heals after replantation.
-
Physiologic storage media include tissue culture media and cell transport media. Examples of osmolality-balanced media are milk and HBSS.
References
-
Fouad AF, Abbott PV, Tsilingaridis G, et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth. Dent Traumatol. 2020;36:331– 342. https://doi.org/10.1111/edt.12573.
-
McDonald and Avery's Dentistry for the Child and Adolescent (11th Edition) -Mosby (2021). https://amzn.to/3vZh9m7
-
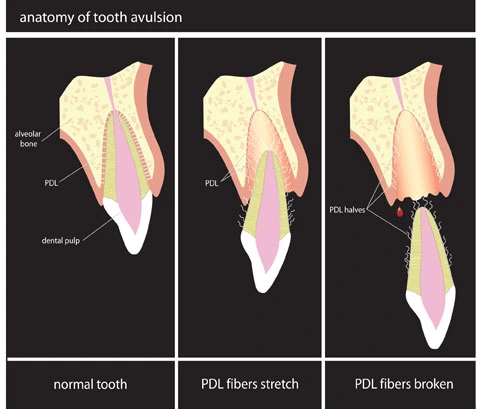
The image used is licensed under the Creative Commons Attribution-Share Alike 3.0 Unported license.
- Description : Diagram showing the way a tooth looks like when it is knocked out of it socket.
- Source : Phoenix-Lazerus, Inc.
- Author : Endsurg.
*This article is an excerpt from the above mentioned books and Medical Sutras does not make any ownership or affiliation claims.