Ameloblastoma is a slow-growing, locally invasive, benign odontogenic tumor of enamel organ type tissue that does not undergo differentiation to the point of enamel formation.
Classification
- Conventional ameloblastoma (80% of cases).
- Unicystic ameloblastoma.
- Extra-osseous/ Peripheral ameloblastoma.
- Metastasizing ameloblastoma.
Origin and Pathogenesis
The cause of ameloblastoma is unknown. However, it likely results from alterations or mutations in the genetic material of cells involved in tooth development. V600E mutation in the BRAF (B-raf proto-oncogene serine/ threonine kinase) gene or mutations of the SMO gene have been identified in ameloblastoma.
Some of the possible sources of origin include :
- Enamel organ.
- Cell rests of enamel organ : Remnants of dental lamina or Remnants of Hertwig's sheath (Epithelial cell rests of Malasez).
- Epithelium of odontogenic cysts (particularly dentigerous cyst) and odontomas.
- Basal cells of the surface epithelium of the jaws.
- Heterotrophic epithelium in other parts of the body, esp. the pituitary gland.
Clinical Features
Ameloblastomas are typically asymptomatic and presents as painless expansion of the jaw.
- More than 80% cases occur in the mandible (angle-ramus area).
- Small lesions : May be found accidentally during routine imaging.
- Large lesions : Can cause jaw expansion, perforation of the cortical plate and even invasion into the surrounding bone. Also, it can lead to significant facial deformity, if left untreated.
Radiographic Features
- Typically, seen as round, cyst-like radiolucent areas with well-defined margins.
- Small lesions : Unilocular.
- Large lesions : Exhibits a compartmented appearance with septa of bone extending into the radiolucent tumor mass. It may consist of a few clustered cysts (soap-bubble multilocularity) or numerous small cysts (honeycomb appearance) or a mixture of patterns.
- Advanced lesion producing jaw expansion, may present as thinning of the cortical plate.
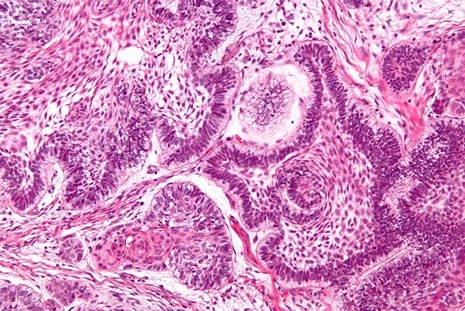
Histologic Features
Conventional ameloblastomas consists of a mixture of solid neoplasm and cysts, where either component may predominate. The solid areas comprise of fibrous tissue containing islands or interconnected strands and sheets of epithelium with a peripheral layer of palisaded preameloblast-like cells.
Six histological subtypes are recognised :
- Follicular
- Plexiform
- Acanthomatous
- Granular cell
- Basal cell
- Desmoplastic
Follicular ameloblastoma
- The solid neoplasm is composed of a peripheral layer of cuboidal or columnar cells enclosing a central mass of polyhedral, loosely arranged cells resembling stellate reticulum.
- Cyst formation is relatively common and occurs due to complete breakdown or cystic degeneration of the stellate reticulum like tissue.
Plexiform ameloblastoma
- The stellate reticulum like tissue is less prominent and cystic degeneration of stroma is common.
Acanthomatous ameloblastoma
- The stellate reticulum like cells undergo squamous metaplasia and are replaced with prickle cells.
- Sometimes, there is keratin formation in the central portion of the tumor islands.
Granular cell ameloblastoma
- The stellate reticulum like cells in the central areas of the tumor islands degenerates and takes a very coarse, granular, eosinophilic appearance.
- These cytoplasmic granules represent lysosomal aggregates with no recognizable cellular components.
- The granular type is an aggressive lesion with a high tendency of recurrence and several cases showing metastasis.
Basal cell ameloblastoma
- The epithelial cells are more primitive and less columnar and consists of darkly staining basal cells, generally arranged in sheets.
- There is little evidence of ameloblast-like cells.
- Bears considerable resemblance with basal cell carcinoma of the skin.
Desmoplastic ameloblastoma
- Characterised by presence of a dense collagen stroma (may appear hyalinised or hypocellular), with the epithelial lining growing in thin strands and cords (compressed and fregmented by the stroma).
- The peripheral cells are often flattened or cuboidal and reverse polarity of nuclei and subnuclear vacoule formation may be difficult to recognise.
Differential Diagnosis
Radiologically ameloblastomas may resemble other lesions of the jaw.
Unilocular ameloblastoma
- Dentigerous cyst.
- Radicular cyst.
- Residual cyst (history of tooth extraction).
- Lateral periodontal cyst (found in incisor, canine and premolar areas in maxilla).
- Giant cell granuloma (occurs anterior to the molar region).
- Traumatic bone cyst (occurs in mid-20s).
- Primordial cyst (occurs in mid-20s).
Multilocular ameloblastoma
- Odontogenic myxoma : History of missing tooth and presence of septa that divide the image into much finer course.
- Odontogenic keratocyst.
- Giant cell granuloma.
Management
The standard treatment for ameloblastoma is wide surgical excision, preferably removing 10 mm of apparently normal surrounding bone (to ensure that any medullary extension is removed).
- Small lesions : Excised, leaving the lower border of the jaw intact and extending the resection sub-periostally.
- Large lesions : Partial jaw resection, often including condyle and bone grafting.
Points to Note
- Other names : Adamantinoma, Adamantoblastoma, Multilocular cyst.
- Adamantinoma was coined by Malassez in 1885, that suggests formation of enamel which is not found in this tumor. The name Ameloblastoma was suggested by Churchil in 1934, that became popular and well accepted.
- Ameloblastoma is the second most common odontogenic tumor, after odontoma.
- Marsupialisation is ineffective and conservative management remains controversial.
References
- Burket's Oral Medicine, 13th Edition, Michael Glick, Martin S. Greenberg, ,Peter B. Lockhart, Stephen J. Challacombe, Wiley Blackwell.
- Shafer, Hine, Levy Shafer's Textbook of Oral Pathology (7th Edition), Editors - R Rajendran, B Sivapathasundharam, Elsevier.
- Cawson's Essentials of Oral Pathology and Oral Medicine, 9th Edition, EW Odell, Elsevier.
- Textbook of Oral Pathology, 2nd Edition, Anil Govindrao Ghom, Shubhangi Mhaske (Jedhe) - Jaypee Brothers Medical Publishers (P) Ltd.
- The image used is licensed under the Creative Commons Attribution-Share Alike 3.0 Unported license (Author: Nephron, Source : Wikimedia Commons).
*This article is an excerpt from the above mentioned books and Medical Sutras does not make any ownership or affiliation claims.