Serious toxicity can occur, If a large dose (more than 150 mg/kg or 10 g in an adult) is taken. Fatality is common with dosage greater than 250 mg/kg.
- Acute paracetamol poisoning occurs especially in small children who have low hepatic glucuronide conjugating ability.
- Chronic alcohol consumption can exacerbate paracetamol toxicity by inducing the liver microsomal enzymes producing the toxic metabolite. In chronic alcoholics, even 5 g taken in one day can result in hepatotoxicity because alcoholism induces CYP2E1 that metabolises paracetamol to NABQI.
Manifestations
- Early manifestations : Nausea, vomiting, abdominal pain and liver tenderness with no impairment of consciousness.
- After 12–18 hours : Centrilobular hepatic necrosis occurs which may be accompanied by renal tubular necrosis and hypoglycemia that may progress to coma.
- Jaundice starts after 2 days.
- Fulminating hepatic failure and death are likely if the plasma levels are high.
Mechanism of Toxicity
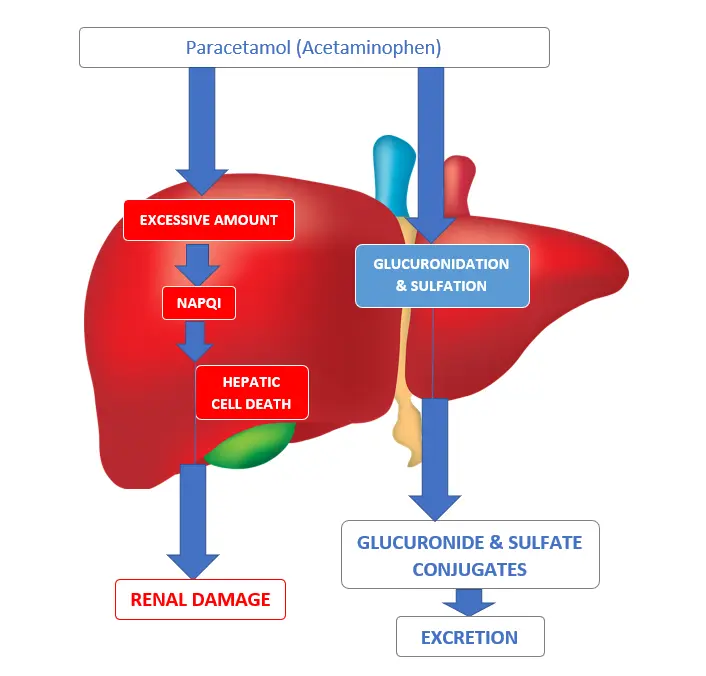
- This occurs when normal conjugation reactions are saturated and the drug is metabolized instead by mixed function oxidases. The resulting toxic metabolite, N-acetyl-p-benzoquinone imine (NABQI) accumulates in the liver and the kidney tubules and causes necrosis.
- N-acetyl-p-benzoquinoneimine (NABQI) is a highly reactive arylating minor metabolite of paracetamol which is detoxified / inactivated by conjugation with glutathione.
- When a very large dose of paracetamol is taken, glucuronidation capacity is saturated and hepatic glutathione is depleted, leading to further formation of the minor metabolite.
- This metabolite binds covalently to proteins in liver cells (and renal tubules) causing necrosis.
- Toxicity, thus shows a threshold effect manifesting only when glutathione is depleted to a critical point.
Treatment
- If the levels are lower - recovery with supportive treatment is the rule.
- If the patient is brought early, vomiting should be induced or gastric lavage done.
- Activated charcoal is given orally or through the tube to prevent further absorption.
- If the patient is seen sufficiently soon after ingestion, the liver damage can be prevented by administering agents that increase glutathione formation in the liver (acetylcysteine intravenously, or methionine orally).
- Specific antidote :
- N-acetylcysteine 150 mg/kg should be infused i.v. in 200 ml of 5% glucose solution over 15 min, followed by the same dose given i.v. over the next 20 hours.
- Alternatively, 75 mg/kg may be given orally every 4–6 hours for 2–3 days.
- It replenishes the glutathione stores of liver and prevents binding of the toxic metabolite to other cellular constituents.
References
- Essentials of Medical Pharmacology 8th Edition (K.D. Tripathi)-Jaypee Brothers Medical Publishers (P) Ltd.
- James Ritter, Rod Flower, Graeme Henderson, Yoon Kong Loke, David MacEwan, Humphrey Rang - Rang & Dale’s Pharmacology-Elsevier (2019).
- Laurence L. Brunton - Goodman & Gilman's Manual of Pharmacology and Therapeutics-McGraw-Hill Medical (2008).
*This article is an excerpt from the above mentioned books and Medical Sutras does not make any ownership or affiliation claims.