Hypoglycemia is the most commonly encountered complication of diabetes.
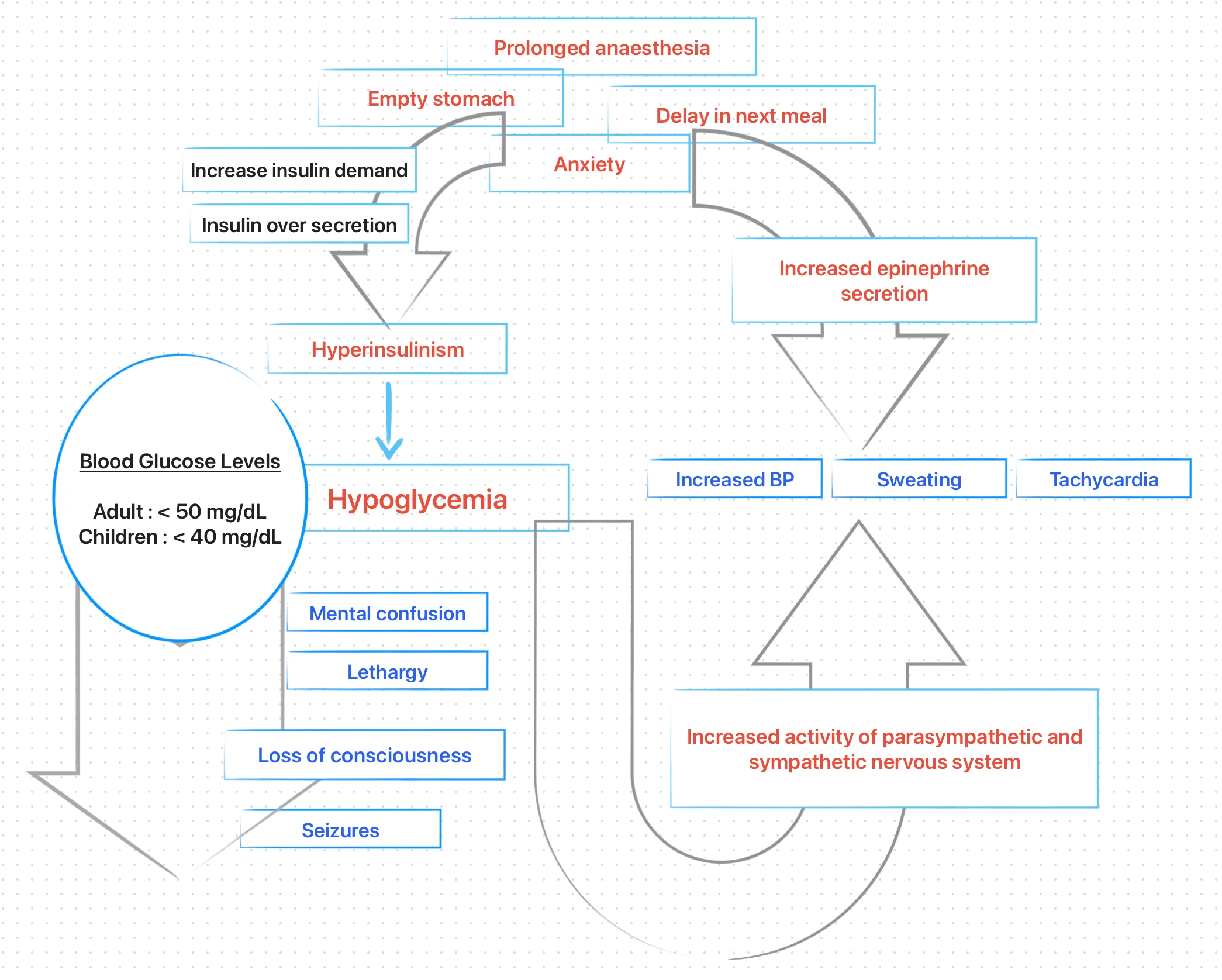
Hypoglycemia occurs when blood glucose level falls below 50 mg/dL in adults and 40 mg/dL in children. However, hypoglycaemic reactions may occur in individuals with normal or higher than normal blood glucose levels.
Pathophysiology
Approximately, 70% of cases of non-diabetic hypoglycemia are caused by functional hyperinsulinism (related to an over secretion of insulin by pancreatic beta cells, due to increase insulin requirements).
Clinical Manifestations
-
Mild (initial symptoms)
- Diminished cerebral function : Inability to perform simple calculations, decreased spontaneity of conversation, and mood change (eg. lethargy).
- CNS involvement : Hunger, nausea, and an increase in gastric motility.
- Weakness.
-
Moderate (sympathetic hyperactivity)
- Increased anxiety, sweating and piloerection.
- Tachycardia.
- Cold and wet skin. (Hyperglycaemia - hot, dry skin).
- Individual is conscious but may exhibit bizarre behavioural patterns such as confusion and uncooperativeness.
-
Severe (further drop in blood glucose levels)
- Hypotension.
- Loss of consciousness.
- Seizures.
Diagnostic clues
- Weakness, dizziness.
- Pale, moist skin.
- Normal or depressed respirations.
- Headache.
- Altered level of consciousness.
Management
The method of management depends on the patient's level of consciousness.
Conscious patient
-
Terminate all dental treatment.
-
Place the patient in a comfortable position. In most situations, the patient prefers to sit upright.
-
Assess circulation, airway and breathing.
-
Administer oral carbohydrates
- If the patient is conscious and cooperative, oral carbohydrates such as sugar, orange juice, soft drinks and candy bars are the treatment of choice.
- The carbohydrate should be administered in 3- or 4 ounce doses every 5-10 minutes until symptoms disappear.
-
Once the patient recovers,
- Observe for approximately 1 hour before discharging the patient.
- Arrangements should be made for a responsible adult to escort the patient home.
If the patient does not respond to oral glucose or cooperate in ingesting,
-
Call for medical assistance.
-
Administer parenteral carbohydrates
- Glucagon (1 mg) may be administered IM or IV (patient usually responds within 10-15 minutes), or,
- 50 mL of a 50% dextrose solution may be administered IV over 2-3 minutes (patient usually responds within 5 minutes).
-
Oral carbohydrates should be started as soon as tolerated by the patient.
-
Monitor vital signs every 5 minutes.
-
Shift to a hospital for evaluation and any further management required.
Unconscious patient
-
Terminate all dental treatment.
-
Place the patient in supine position with legs elevated slightly.
-
Assess circulation, airway and breathing and start BLS, as needed. Usually circulation is adequate and breathing is spontaneous, and the patient requires only airway management.
-
Call for medical assistance.
-
Administer carbohydrates :
- 50% dextrose solution IV or glucagon (1 mg) IM or IV.
- Oral administration : Any liquid or other substance such as gel or paste (that can liquefy at body temperature) should never be given to an unconscious patient orally : The substance might run down into the throat and increase the possibility of aspiration or airway obstruction.
-
If neither glucagon nor a 50% dextrose solution is available, 0.5 mg of a 1:1000 epinephrine concentration may be administered via the subcutaneous or IM route and repeated every 15 minutes as needed.
-
Severe hypoglycemia may be associated with the development of generalised tonic-clonic seizures : Managed same as other seizures. (*Seizures induced by hypoglycemia may persist until the blood glucose levels increases).
-
Shift the patient to a hospital for definitive care and observation.
References
- Medical Emergencies in the Dental Practice (7th edition), Stanley F. Malamed, Daniel L Orr II, Mosby Elsevier.
- Contemporary Oral and Maxillofacial Surgery (6th edition), James R Hupp, Edward Ellis III, Myron R Tucker, Mosby Elsevier.
*This article is an excerpt from the above mentioned books and Medical Sutras does not make any ownership or affiliation claims.