Though uncommon, acute adrenal insufficiency is a potentially life threatening medical emergency, that can occur in patients undergoing stressful dental treatment (such as surgical extraction of impacted third molars), and having little-to-no adrenal function (due to primary or secondary adrenal insufficiency).
Primary vs Secondary Adrenal Insufficiency
Primary adrenocortical insufficiency (Addison's disease)
- There is autoimmune destruction of the adrenal glands (80% of cases).
- Clinical manifestations of the adrenal insufficiency usually develops when 90% of the adrenal cortex is destroyed.
Secondary adrenal insufficiency
- There is hypofunction of the adrenal glands due to administration of exogenous glucocorticoids in patients with normal, functional adrenal cortices.
- Glucocorticoids administered in pharmacologic doses produces a disuse atrophy of the adrenal cortex and decreases its ability to increase corticosteroid levels in response to stressful situations.
Pathophysiology
The major predisposing factor is the lack of glucocorticoid hormones. This may result due to several reasons :
- Sudden withdrawal of steroids in patients suffering from primary or secondary adrenal insufficiency.
- Physiologic or Psychological stress, that require high levels of glucocorticoid in the system.
- Bilateral adrenalectomy or removal of a functioning adrenal tumor suppressing the the other adrenal gland.
- Sudden destruction of the pituitary gland.
- Injury to the adrenal glands due to trauma, haemorrhage, infection, thrombosis, or tumor.
Clinical Manifestations
Early Manifestations
- Mental confusion.
- Nausea.
- Fatigue.
- Myalgia and weakness.
Late Manifestations
- More severe mental confusion.
- Pain in the back, abdomen and legs.
- Vomiting.
- Hypotension.
- Unconsciousness (partial or total) and coma.
Adrenal Insufficiency
- Symptoms : Weakness, fatigue, Anorexia, Gastrointestinal symptoms, Weight loss, Hyponatremia, Hypotension (BP less than or equal to 110/70), Mild fever, Depression, apathy.
- Primary Signs : Hyperpigmentation, Salt craving, Hyperkalemia, Hyperchloremia, Orthostasis (Syncope), Vitiligo.
- Secondary Signs : Hypoglycemia, Amenorrhea.
Management
-
Terminate all dental procedures.
-
Positioning
- Supine position with the legs raised above the head level, if the patient appears mentally confused, wet and clammy (hypotensive).
- However, if the patient does not exhibit any of these signs and symptoms, position the patient according to comfort.
-
Assess Circulation-Airway-Breathing.
-
Monitor vital signs every 5 minutes.
-
Call for medical assistance.
-
Administer corticosteroid :
- If the patient shows signs and symptoms of acute adrenal insufficiency and have prior history of adrenal insufficiency or is using glucocorticoids.
- Hydrocortisone (50-100mg) IM (Vastus lateralis or mid-deltoid area) or IV (over 30 seconds) : Re-administered every 6-8 hours.
- Dexamethasone phosphate (4mg) IV every 6-8 hours.
- Indicated immediately, while awaiting ACTH stimulation test.
-
Administer Oxygen (5-10 litres per minute).
-
Administer IV fluids : 1 L of normal saline (for hypotension), followed by 5% dextrose (in case of low blood glucose levels, 45 mg/dL).
-
Start BLS, if there is loss of consciousness.
-
Shift the patient to an emergency care facility.
Points to Note
-
Patients with secondary adrenal insufficiency are in more danger to develop acute adrenal crisis than those with Addison's disease.
-
Acute adrenal insufficiency should be suspected in patients who :
- Exhibit mental confusion, nausea, vomiting and abdominal pain, and
- Are under glucocorticoid therapy or have recently ceased long-term corticosteroid therapy.
-
ACTH stimulation test
- Laboratory test to confirm adrenal insufficiency.
- 0.25mg Cosyntropin (synthetic ACTH) is administered at time 0, followed by serum samples taken at time 0, 1 hour and 6-8 hours.
- Normal adrenal glands respond with increase in cortisol to at least 10mg/fl or three times the baseline level.
-
Dexamethasone is approximately 100 times more potent than cortisol.
References
-
Medical Emergencies in the Dental Practice (7th Edition), Stanley F. Malamed, Daniel L Orr II, Mosby Elsevier. https://amzn.to/4bsbBkf
-
Contemporary Oral and Maxillofacial Surgery (6th Edition), James R Hupp, Edward Ellis III, Myron R Tucker, Mosby Elsevier. https://amzn.to/3HJehMO
-
The image used is licensed under the Creative Commons Attribution-Share Alike 4.0 International license.
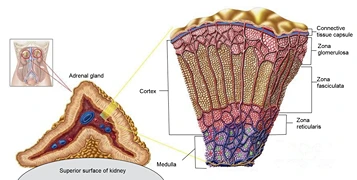
- Description : Depiction of location of adrenal glands in human body; zoom to detail of adrenal gland; zoom to cross section of adrenal gland; cross section shows cortex, including connective tissue capsule, zona glomerulosa, zona fasciculata, and zona reticularis; also shows medulla.
- Source : https://commons.wikimedia.org/wiki/File:Antinks%C4%8Dio_sandara_esp.png
- Author : Antinksčio sandara.png Author: EdgarasLe.
{kind=link}
*This article is an excerpt from the above mentioned books and Medical Sutras does not make any ownership or affiliation claims.