Direct retainers are those components of a removable partial denture that are used to retain and prevent dislodgement, and consist of a clasp assembly or precision attachment.
Classification/Types of Direct Retainers
-
Intracoronal retainers
- Precision attachments
- Semi-precision attachments
-
Extracoronal retainers
- Extracoronal attachments
- Retentive clasp assemblies: Suprabulge & Infrabulge
Intracoronal Direct Retainers
An intracoronal direct retainer resides within the normal contours of an abutment and functions to retain and stabilize a removable partial denture.
-
The first intracoronal direct retainer was introduced by Herman E. S. Chayes in 1906.
-
It consists of:
- Matrix: A metal receptacle contained within the normal clinical contours of a fixed restoration.
- Patrix: Attached to the corresponding removable partial denture.
-
Parallelism of matrix and patrix results in a well-defined path of insertion and removal and in mechanical binding when off-axis forces are applied to the prosthesis.
-
Based on the method of fabrication and tolerance of fit between components, intracoronal direct retainers can be subdivided into two categories:
- Precision attachments, and
- Semi-precision attachments.
Precision Attachments
- Components are fabricated in metal using high-precision manufacturing techniques.
- These attachments usually exhibit long, parallel walls and exceptional surface adaptation.
Semi-precision Attachments
- Components usually originate as wax or plastic patterns, which are subsequently cast in metal.
- Unlike precision attachments, these often have gently tapering walls.
- Displays a less intimate fit between matrix and patrix components.
Extracoronal Direct Retainers
These consist of components that reside entirely outside the normal clinical contours of abutment teeth, and can be divided into two distinct subcategories
- Extracoronal attachments, and
- Retentive clasp assemblies.
Extracoronal Attachments
- These were first introduced by Henry R. Boos in the early 1900s and were later modified by F. Ewing Roach (1908).
- They derive their retention from closely fitting components termed matrices and patrices.
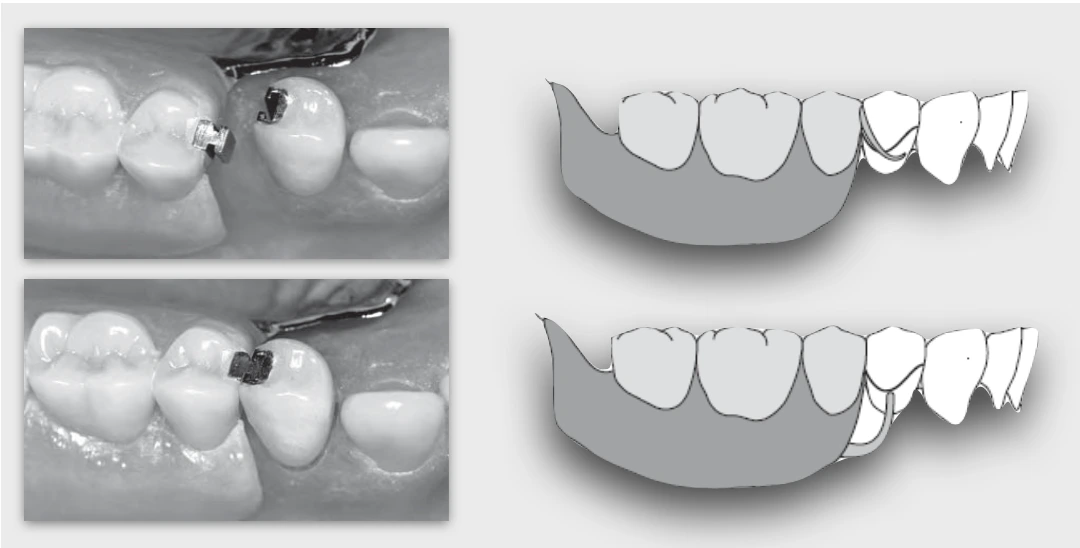
- Many of these attachments permit vertical movement of prostheses during occlusal loading. This mechanical accommodation is intended to minimize the transfer of potentially damaging forces to the abutments. This concept has led to “stress breaking” or “stress directing” theories of removable partial denture design.
Retentive Clasp Assemblies
-
Clasp: The component of the clasp assembly that engages a portion of the tooth surface and either enters an undercut for retention or remains entirely above the height of contour to act as a reciprocating element; generally it is used to stabilize and retain a removable partial denture. (GPT 9)
-
To understand the mechanics of such a retainer, the practitioner must understand two important concepts—
- Path of insertion and removal for the prosthesis: The specific direction in which a prosthesis is placed on the residual alveolar ridge, abutment teeth, dental implant abutment(s), or attachments. (GPT9)
- Height of contour for each abutment: A line encircling a tooth and designating its greatest circumference at a selected axial position determined by a dental surveyor; a line encircling a body designating its greatest circumference in a specified plane. (GPT-9)
Types of Retentive Clasp Assemblies
-
Suprabulge clasp assembly
- Suprabulge clasp is any removable partial denture retentive clasp that approaches the retentive undercut from an occlusal or suprabulge direction.
- Suprabulge area is that portion of a tooth or crown that converges toward the occlusal surface, i.e., above the height of contour
-
Infrabulge clasp assembly
- Infrabulge clasp is defined as a removable partial denture retentive clasp that approaches the retentive undercut from a cervical or infrabulge direction.
- Infrabulge area is that portion of the crown of a tooth apical to the survey line.
Points to Note
- Cone Theory of Clinical Crown Anatomy: It was introduced by J. H. Prothero in 1916, and provided a conceptual basis for mechanical retention. According to Prothero’s explanation, the contours of a clinical crown resemble two cones sharing a common base. The line formed at the junction of these cones represents the greatest diameter of the tooth. This diameter is commonly referred to as the height of contour*,* a term first used by Dr Edward Kennedy in 1928.
- Upon insertion, the clasp arms will contact the axial surfaces of the abutment. With continued seating, the retentive clasp arms will flex as they pass over the greatest convexities of the abutments. Once the point of greatest tooth convexity is reached, further placement of the prosthesis allows each retentive clasp arm to return to its “unstrained” or “passive” state. This places the retentive terminus in an undercut relative to the path of insertion and removal.
References
- Stewart’s Clinical Removable Partial Prosthodontics (4th edition), Rodney D. Phoenix, David R. Cagna, Charles F. DeFreest, Quintessence Books.
- McCracken’s Removable Partial Prosthodontics (13th edition), Alan B. Carr DMD MS, David T. Brown DDS MS, Elsevier.
- Glossary of Prosthodontic Terms-9
*This article is an excerpt from the above mentioned books and Medical Sutras does not make any ownership and affiliation claims.